

A complications-based clinical staging of obesity to guide treatment modality and intensity
- PMID: 23974764
- PMCID: PMC4139285
- DOI: 10.1097/01.med.0000433067.01671.f5
A complications-based clinical staging of obesity to guide treatment modality and intensity
Abstract
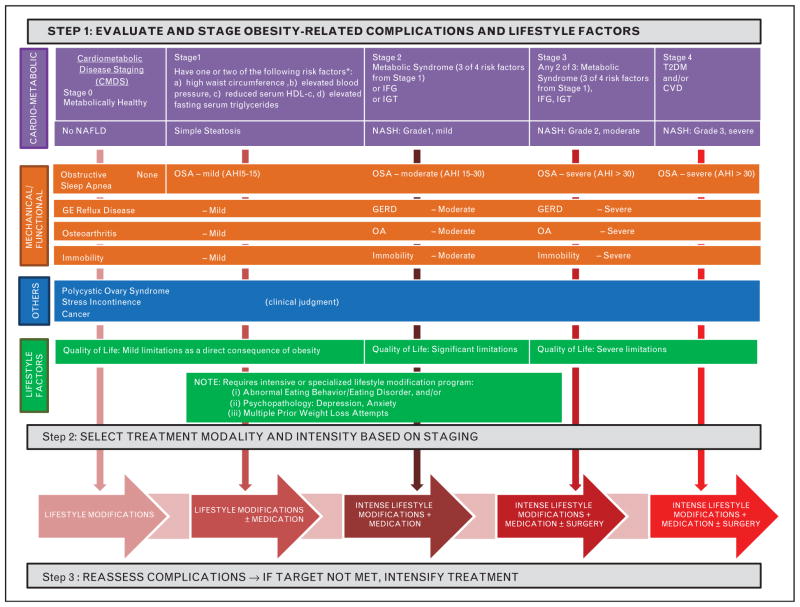
Purpose of review: The current medical model for obesity management is BMI-centric because BMI is the predominant measure used to gauge disease severity, as well as indications for various treatment modalities. Recent advancements in therapy and understanding of the relationship between BMI and obesity-related complications call for a re-examination of this approach.
Recent findings: Advancements in treatment, including the recent approval of two new weight loss medications in the USA, have enabled development of new medical models for management of obesity. On the basis of accumulating data demonstrating the benefits of weight loss regarding multiple obesity-related complications (e.g., diabetes prevention, type 2 diabetes mellitus, cardiovascular disease risk, nonalcoholic steatohepatitis, sleep apnea), a complications-centric model is proposed that employs weight loss as a tool to treat and prevent obesity comorbidities. This model assures that the aggressiveness of therapy is commensurate with disease severity, and that therapy is directed at those obese patients who will benefit most from weight loss therapy. The treatment algorithm is comprehensive in addressing complications and quantitative when possible in the staging of risk or disease severity.
Summary: A complications-centric approach to obesity management identifies patients who will benefit most from weight loss, and optimizes patient outcomes, benefit/risk ratio, and the cost-effectiveness of interventions.
Conflict of interest statement
This work was supported by the Merit Review program of the Department of Veterans Affairs, the National Institutes of Health (DK-038765 and DK-083562), and the UAB Diabetes Research Center (P60-DK079626).
W.T.G. is a speaker for Merck, Amylin, and Liposcience. He is on the advisory boards of Daiichi-Sankyo, Vivus, Alkermes, Eisai, Liposcience, Tethys Bioscience, and Janssen. He receives research support from Merck, Amylin, and Weight Watchers. S.D. is a speaker for Vivus. T.S. is a speaker for Vivus.
Figures
References
-
- Mechanick JI, Garber AJ, Handelsman Y, Garvey WT. American Association of Clinical Endocrinologists’ position statement on obesity and obesity medicine. Endocr Pract. 2012;18:642–648. This article articulates that the American Association of Clinical Endocrinologists considers obesity to be a disease and provides supportive rationale. These arguments led the American Medical Association to subsequently designate obesity as a disease in 2013. - PubMed
-
- Kushner RF, Sarwer DB. Medical and behavioral evaluation of patients with obesity. Psychiatr Clin N Am. 2011;34:797–812. - PubMed
-
- Flegal KM, Carroll MD, Ogden CL, et al. Prevalence and trends in obesity among US adults, 1999–2008. JAMA. 2010;303:235–241. - PubMed
-
- Ogden CL, Carroll MD, Curtin LR, et al. Prevalence of high body mass index in US children and adolescents, 2007–2008. JAMA. 2010;303:242–249. - PubMed
-
- NHLBI Obesity Education Initiative Expert Panel on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults. Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults: the evidence report. Obes Res. 1998;6:51S–209S. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
