

Infection after surgical resection for pelvic bone tumors: an analysis of 270 patients from one institution
- PMID: 23975252
- PMCID: PMC3889428
- DOI: 10.1007/s11999-013-3250-x
Infection after surgical resection for pelvic bone tumors: an analysis of 270 patients from one institution
Abstract
Background: Surgical treatment of pelvic tumors with or without acetabular involvement is challenging. Primary goals of surgery include local control and maintenance of good quality of life, but the procedures are marked by significant perioperative morbidity and complications.
Questions/purposes: We wished to (1) evaluate the frequency of infection after limb salvage surgical resection for bone tumors in the pelvis; (2) determine whether infection after these resections is associated with particular risk factors, including pelvic reconstruction, radiotherapy or chemotherapy, type of resection, and age; and (3) analyze treatment of these infections, particularly with respect to the need of additional surgery or hemipelvectomy.
Methods: From 1975 to 2010, 270 patients with pelvic bone tumors (149 with chondrosarcoma, 40 with Ewing's sarcoma, 27 with osteosarcoma, 18 with other primary malignant tumors, 11 with metastatic tumors, and 25 with primary benign tumors) were treated by surgical resection. Minimum followup was 1.1 years (mean, 8 years; range, 1-33 years). The resection involved the periacetabular area in 166 patients. In 137 patients reconstruction was performed; in 133 there was no reconstruction. Chart review ascertained the frequency of deep infections, how they were treated, and the frequency of resection arthroplasty or hemipelvectomies that occurred thereafter.
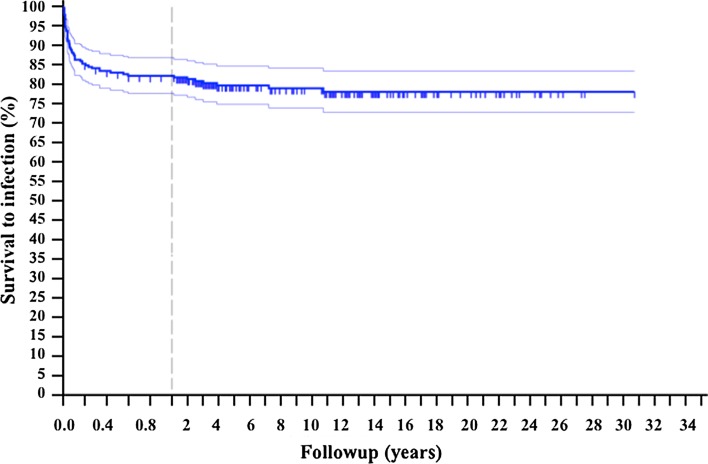
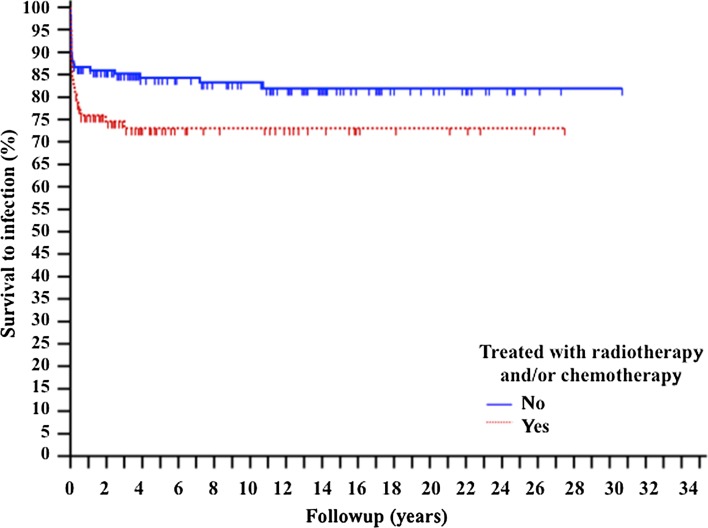
Results: A total of 55 patients (20%) had a deep infection develop at a mean followup of 8 months. There were 20 infections in 133 patients without reconstruction (15%) and 35 infections in 137 patients with reconstruction (26 %). Survivorship rates of the index procedures using infection as the end point were 87%, 83%, and 80% at 1 month, 1 year, and 5 years, respectively. Infection was more common in patients who underwent pelvic reconstruction after resection (univariate analysis, p = 0.0326; multivariate analysis, p = 0.0418; odds ratio, 1.7718; 95% CI, 1.0243-3.0650); no other risk factors we evaluated were associated with an increased likelihood of infection. Despite surgical débridements and antibiotics, 16 patients (46%) had the implant removed and five (9%) underwent external hemipelvectomy (four owing to infection and one as a result of persistent infection and local recurrence).
Conclusions: Infection is a common complication of pelvic resection for bone tumors. Reconstruction after resection is associated with an increased risk of infection compared with resection alone, without significant difference in percentage between allograft and metallic prosthesis. When infection occurs, it requires removal of the implant in nearly half of the patients who have this complication develop, and external hemipelvectomy sometimes is needed to eradicate the infection.
Figures



References
-
- Aboulafia AJ, Buch R, Mathews J, Li W, Malawer MM. Reconstruction using the saddle prosthesis following excision of primary and metastatic periacetabular tumors. Clin Orthop Relat Res. 1995;314:203–213. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
