

Axillary dissection can be avoided in the majority of clinically node-negative patients undergoing breast-conserving therapy
- PMID: 23975314
- PMCID: PMC4349525
- DOI: 10.1245/s10434-013-3200-6
Axillary dissection can be avoided in the majority of clinically node-negative patients undergoing breast-conserving therapy
Abstract
Background: The extent to which ACOSOG Z0011 findings are applicable to patients undergoing breast-conserving therapy (BCT) is uncertain. We prospectively assessed how often axillary dissection (ALND) was avoided in an unselected, consecutive patient cohort meeting Z0011 eligibility criteria and whether subgroups requiring ALND could be identified preoperatively.
Methods: Patients with cT1,2cN0 breast cancer undergoing BCT were managed without ALND for metastases in <3 sentinel nodes (SNs) and no gross extracapsular extension (ECE). Patients with and without indications for ALND were compared using Fisher's exact and Wilcoxon rank sum tests.
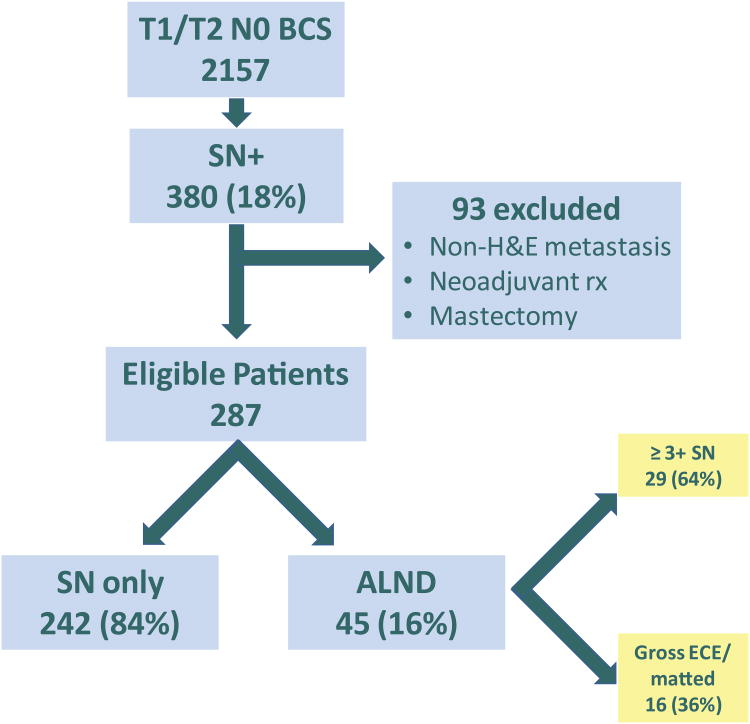
Results: From August 2010 to November 2012, 2,157 invasive cancer patients had BCT. A total of 380 had histologic nodal metastasis; 93 did not meet Z0011 criteria. Of 287 with ≥1 H&E-positive SN (209 macrometastases), 242 (84 %) had indications for SN only. ALND was indicated in 45 for ≥3 positive SNs (n = 29) or ECE (n = 16). The median number of SNs removed in the SN group was 3 versus 5 in the ALND group (p < 0.0001). Age, hormone receptor and HER2 status, and grade did not differ between groups; tumors were larger in the ALND group (p < 0.0001). Of ALND patients, 72 % had additional positive nodes (median = 1; range 1-19). No axillary recurrences have occurred (median follow-up, 13 months).
Conclusions: ALND was avoided in 84 % of a consecutive series of patients having BCT, suggesting that most patients meeting ACOSOG Z0011 eligibility have a low axillary tumor burden. Age, ER, and HER2 status were not predictive of ALND, and the criteria used for ALND (≥3 SNs, ECE) reliably identified patients at high risk for residual axillary disease.
Conflict of interest statement
Figures

Comment in
-
Axillary dissection can be avoided in the majority of clinically node-negative patients undergoing breast-conserving therapy, by Dengel et al.Ann Surg Oncol. 2014 Jan;21(1):8-10. doi: 10.1245/s10434-013-3201-5. Epub 2013 Aug 22. Ann Surg Oncol. 2014. PMID: 23975315 No abstract available.
References
-
- Giuliano AE, McCall L, Beitsch P, et al. Locoregional recurrence after sentinel lymph node dissection with or without axillary dissection in patients with sentinel lymph node metastases: the American College of Surgeons Oncology Group Z0011 randomized trial. Ann Surg. 2010;252(3):426–32. discussion 32-3. - PMC - PubMed
-
- Sneige N, Wang J, Baker BA, et al. Clinical, histopathologic, and biologic features of pleomorphic lobular (ductal-lobular) carcinoma in situ of the breast: a report of 24 cases. Mod Pathol. 2002;15(10):1044–50. - PubMed
-
- Giuliano AE, Morrow M, Duggal S, et al. Should ACOSOG Z0011 change practice with respect to axillary lymph node dissection for a positive sentinel lymph node biopsy in breast cancer? Clin Exp Metastasis. 2012;29(7):687–92. - PubMed
-
- Shah-Khan M, Boughey JC. Evolution of axillary nodal staging in breast cancer: clinical implications of the ACOSOG Z0011 trial. Cancer Control. 2012;19(4):267–76. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
