

Risk of early-onset neonatal infection with maternal infection or colonization: a global systematic review and meta-analysis
- PMID: 23976885
- PMCID: PMC3747995
- DOI: 10.1371/journal.pmed.1001502
Risk of early-onset neonatal infection with maternal infection or colonization: a global systematic review and meta-analysis
Abstract
Background: Neonatal infections cause a significant proportion of deaths in the first week of life, yet little is known about risk factors and pathways of transmission for early-onset neonatal sepsis globally. We aimed to estimate the risk of neonatal infection (excluding sexually transmitted diseases [STDs] or congenital infections) in the first seven days of life among newborns of mothers with bacterial infection or colonization during the intrapartum period.
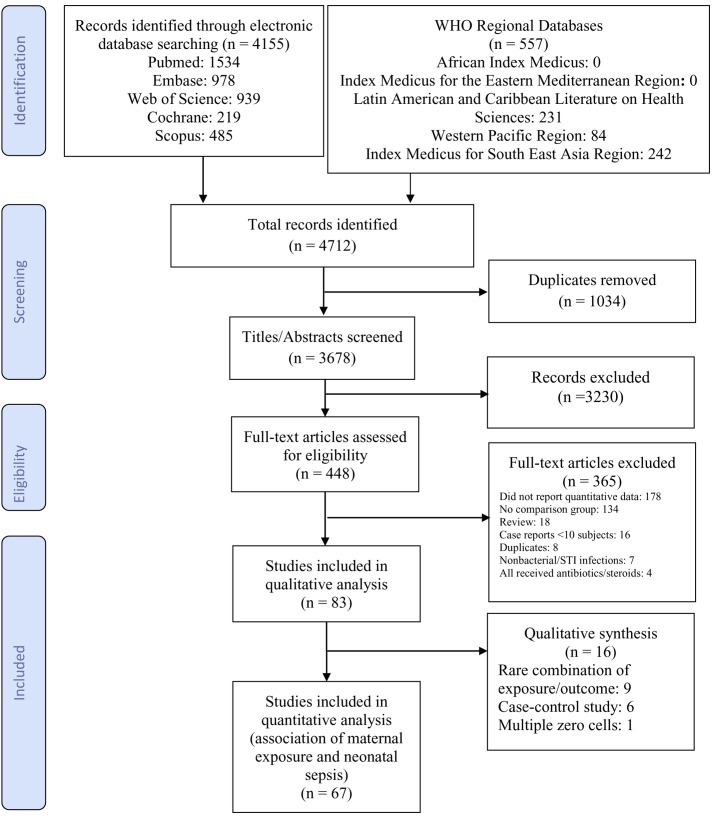
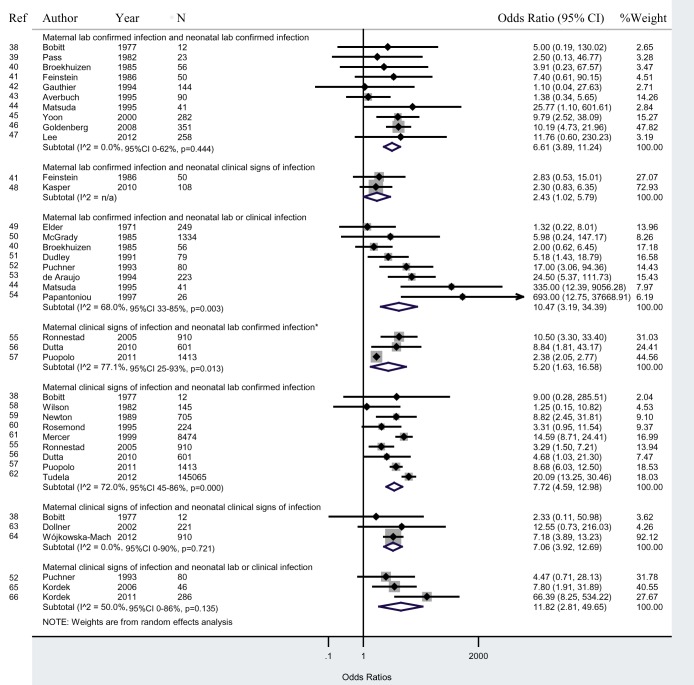
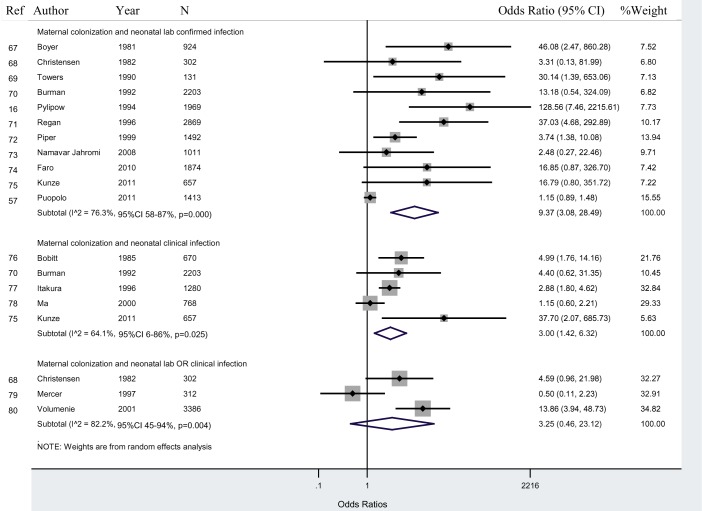
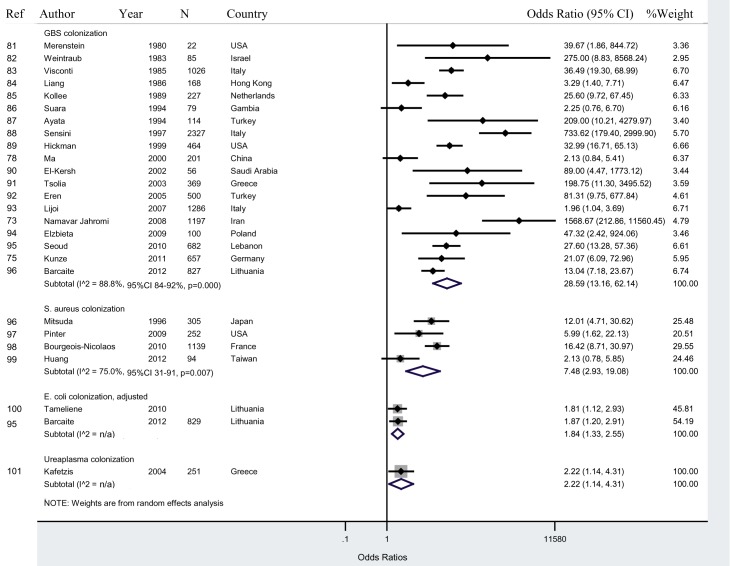
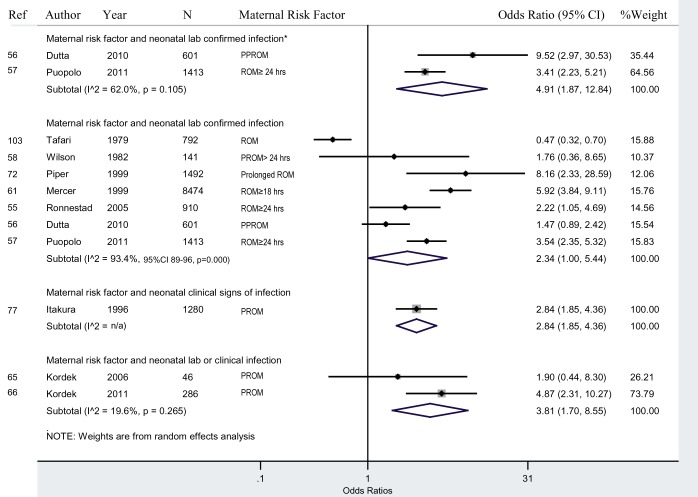
Methods and findings: We searched PubMed, Embase, Scopus, Web of Science, Cochrane Library, and the World Health Organization Regional Databases for studies of maternal infection, vertical transmission, and neonatal infection published from January 1, 1960 to March 30, 2013. Studies were included that reported effect measures on the risk of neonatal infection among newborns exposed to maternal infection. Random effects meta-analyses were used to pool data and calculate the odds ratio estimates of risk of infection. Eighty-three studies met the inclusion criteria. Seven studies (8.4%) were from high neonatal mortality settings. Considerable heterogeneity existed between studies given the various definitions of laboratory-confirmed and clinical signs of infection, as well as for colonization and risk factors. The odds ratio for neonatal lab-confirmed infection among newborns of mothers with lab-confirmed infection was 6.6 (95% CI 3.9-11.2). Newborns of mothers with colonization had a 9.4 (95% CI 3.1-28.5) times higher odds of lab-confirmed infection than newborns of non-colonized mothers. Newborns of mothers with risk factors for infection (defined as prelabour rupture of membranes [PROM], preterm <37 weeks PROM, and prolonged ROM) had a 2.3 (95% CI 1.0-5.4) times higher odds of infection than newborns of mothers without risk factors.
Conclusions: Neonatal infection in the first week of life is associated with maternal infection and colonization. High-quality studies, particularly from settings with high neonatal mortality, are needed to determine whether targeting treatment of maternal infections or colonization, and/or prophylactic antibiotic treatment of newborns of high risk mothers, may prevent a significant proportion of early-onset neonatal sepsis. Please see later in the article for the Editors' Summary.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Liu L, Johnson HL, Cousens S, Perin J, Scott S, et al. (2012) Global, regional, and national causes of child mortality: an updated systematic analysis for 2010 with time trends since 2000. Lancet 379: 2151–2161. - PubMed
-
- Oestergaard MZ, Inoue M, Yoshida S, Mahanani WR, Gore FM, et al. (2011) Neonatal mortality levels for 193 countries in 2009 with trends since 1990: a systematic analysis of progress, projections, and priorities. PLoS Med 8: e1001080 doi:10.1371/journal.pmed.1001080 - DOI - PMC - PubMed
-
- Lawn JE, Lee AC, Kinney M, Sibley L, Carlo WA, et al. (2009) Two million intrapartum-related stillbirths and neonatal deaths: where, why, and what can be done? Int J Gynaecol Obstet 107 Suppl 1: S5–18, S19. - PubMed
-
- Al-Adnani M, Sebire NJ (2007) The role of perinatal pathological examination in subclinical infection in obstetrics. Best Pract Res Clin Obstet Gynaecol 21: 505–521. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
