

The effectiveness of inodilators in reducing short term mortality among patient with severe cardiogenic shock: a propensity-based analysis
- PMID: 23977106
- PMCID: PMC3744474
- DOI: 10.1371/journal.pone.0071659
The effectiveness of inodilators in reducing short term mortality among patient with severe cardiogenic shock: a propensity-based analysis
Erratum in
- PLoS One. 2013;8(12). doi:10.1371/annotation/add6bc4f-dec0-4c95-a609-67563469b831
Abstract
Background: The best catecholamine regimen for cardiogenic shock has been poorly evaluated. When a vasopressor is required to treat patients with the most severe form of cardiogenic shock, whether inodilators should be added or whether inopressors can be used alone has not been established. The purpose of this study was to compare the impact of these two strategies on short-term mortality in patients with severe cardiogenic shocks.
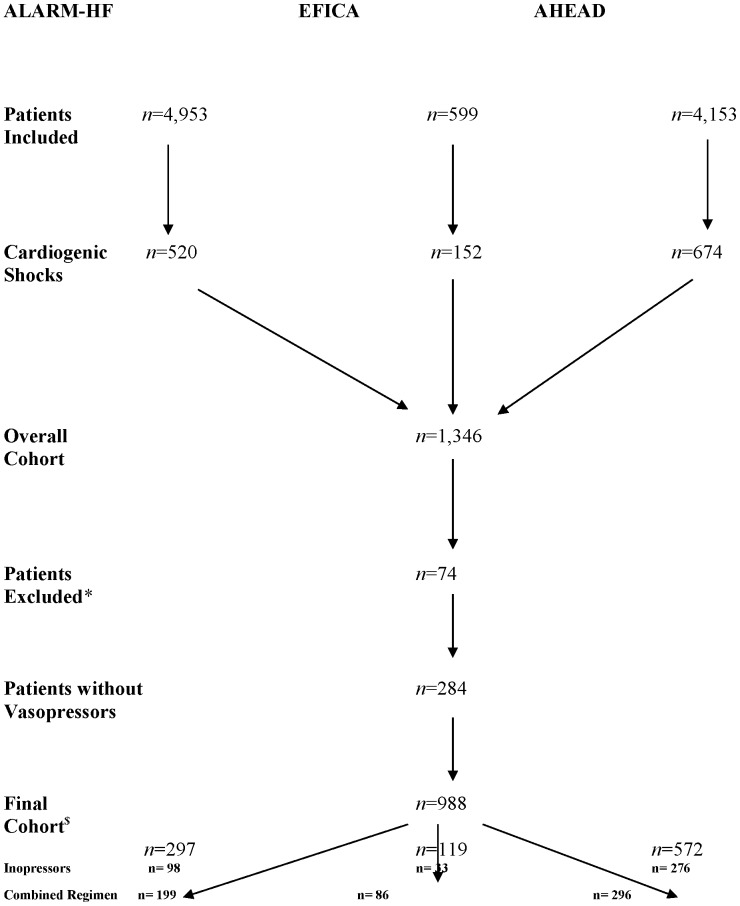
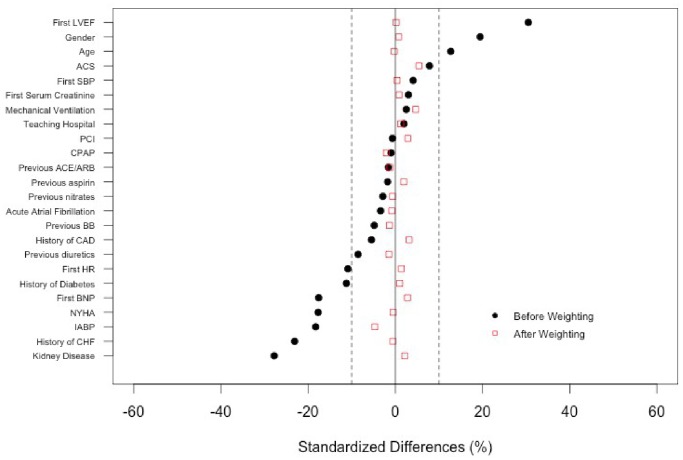
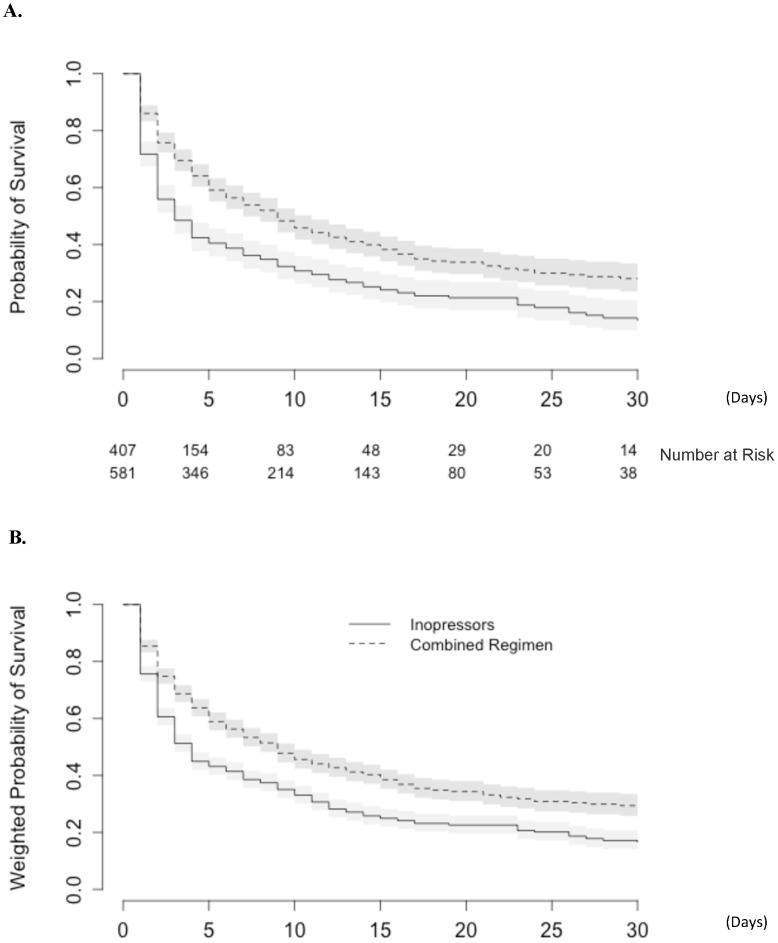
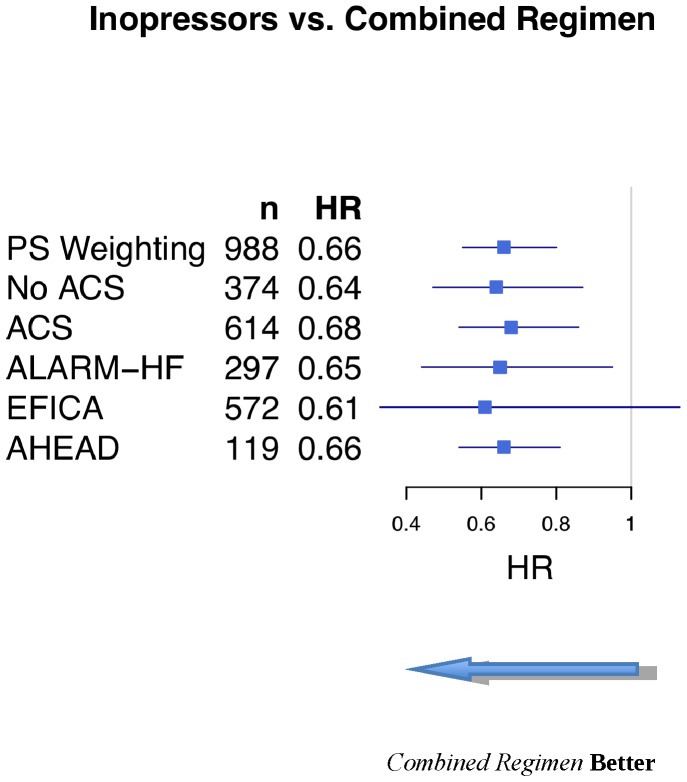
Methods and results: Three observational cohorts of patients with decompensated heart failure were pooled to comprise a total of 1,272 patients with cardiogenic shocks. Of these 1,272 patients, 988 were considered to be severe because they required a vasopressor during the first 24 hours. We developed a propensity-score (PS) model to predict the individual probability of receiving one of the two regimens (inopressors alone or a combination) conditionally on baseline-measured covariates. The benefit of the treatment regimen on the mortality rate was estimated by fitting a weighted Cox regression model. A total of 643 patients (65.1%) died within the first 30 days (inopressors alone: 293 (72.0%); inopressors and inodilators: 350 (60.0%)). After PS weighting, we observed that the use of an inopressor plus an inodilator was associated with an improved short-term mortality (HR: 0.66 [0.55-0.80]) compared to inopressors alone.
Conclusions: In the most severe forms of cardiogenic shock where a vasopressor is immediately required, adding an inodilator may improve short-term mortality. This result should be confirmed in a randomized, controlled trial.
Conflict of interest statement
Figures
References
-
- Krenn L, Delle Karth G (2011) Essential lessons in cardiogenic shock: epinephrine versus norepinephrine/dobutamine. Crit Care Med 39: 583–584 doi:10.1097/CCM.0b013e318208e381 - DOI - PubMed
-
- McMurray JJV, Adamopoulos S, Anker SD, Auricchio A, Böhm M, et al. (2012) ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur Heart J 33: 1787–1847 doi:10.1093/eurheartj/ehs104 - DOI - PubMed
-
- Krejci V, Hiltebrand LB, Sigurdsson GH (2006) Effects of epinephrine, norepinephrine, and phenylephrine on microcirculatory blood flow in the gastrointestinal tract in sepsis. Crit Care Med 34: 1456–1463 doi:10.1097/01.CCM.0000215834.48023.57 - DOI - PubMed
-
- Thompson RB, van den Bos EJ, Esposito DJ, Owen CH, Glower DD (2003) The effects of acute afterload change on systolic ventricular function in conscious dogs with normal vs. failing hearts. Eur J Heart Fail 5: 741–749. - PubMed
-
- Capomolla S, Pozzoli M, Opasich C, Febo O, Riccardi G, et al. (1997) Dobutamine and nitroprusside infusion in patients with severe congestive heart failure: hemodynamic improvement by discordant effects on mitral regurgitation, left atrial function, and ventricular function. Am Heart J 134: 1089–1098. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
