

The β-blocker Nebivolol Is a GRK/β-arrestin biased agonist
- PMID: 23977191
- PMCID: PMC3748024
- DOI: 10.1371/journal.pone.0071980
The β-blocker Nebivolol Is a GRK/β-arrestin biased agonist
Abstract
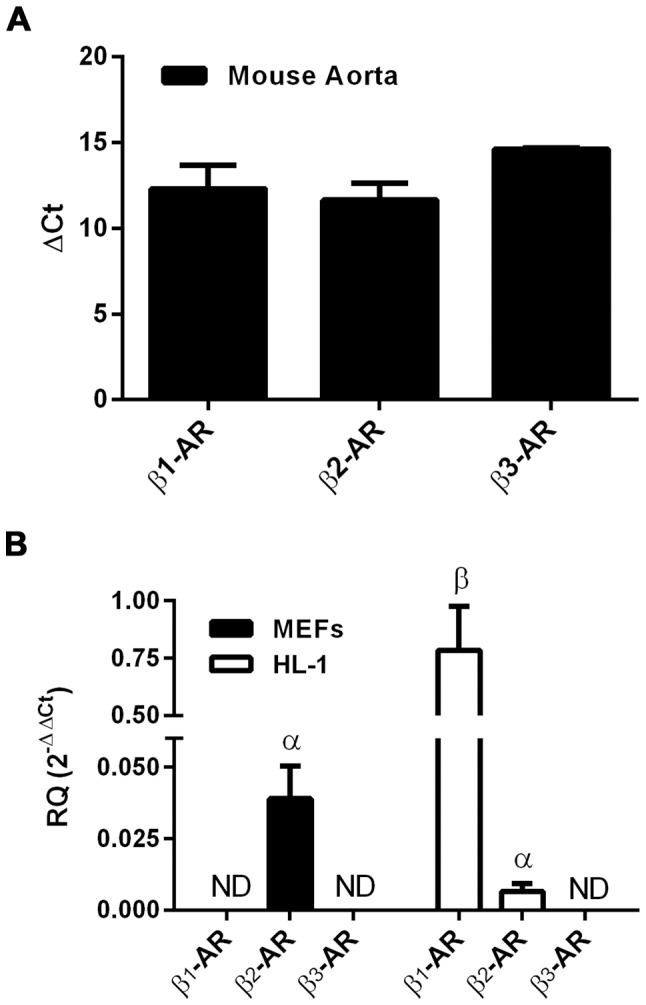
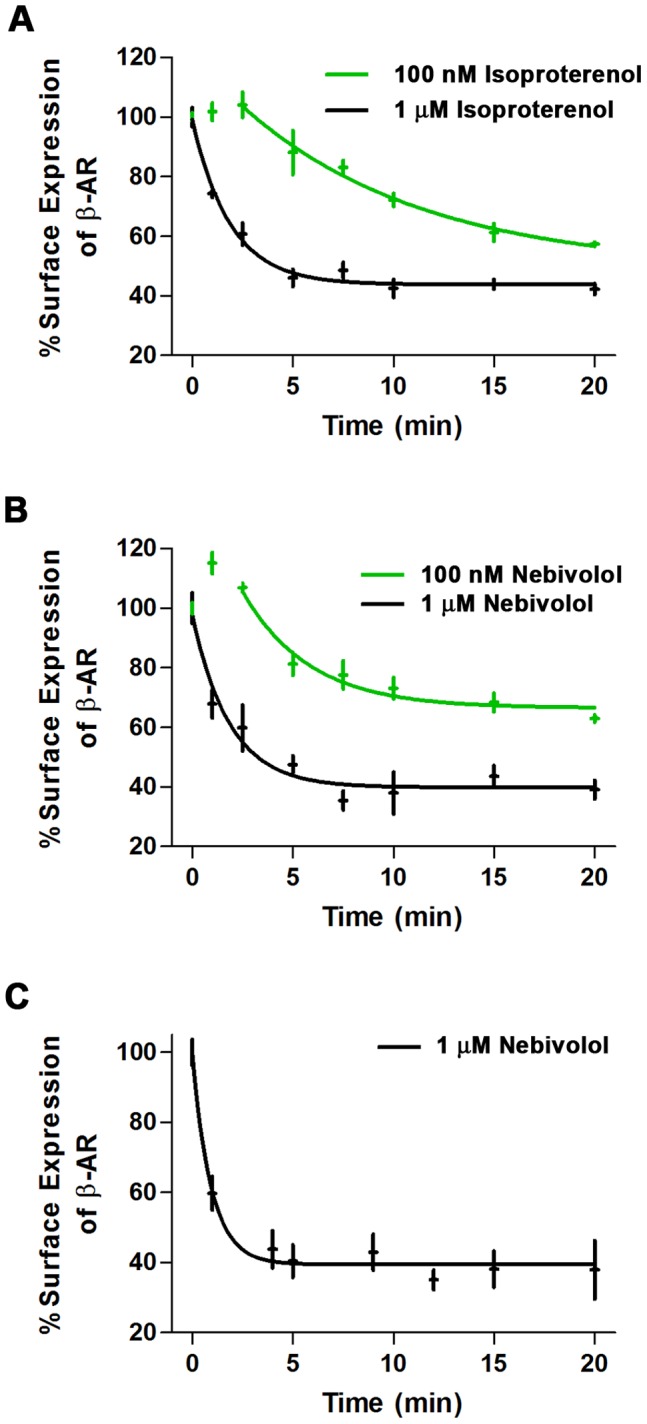
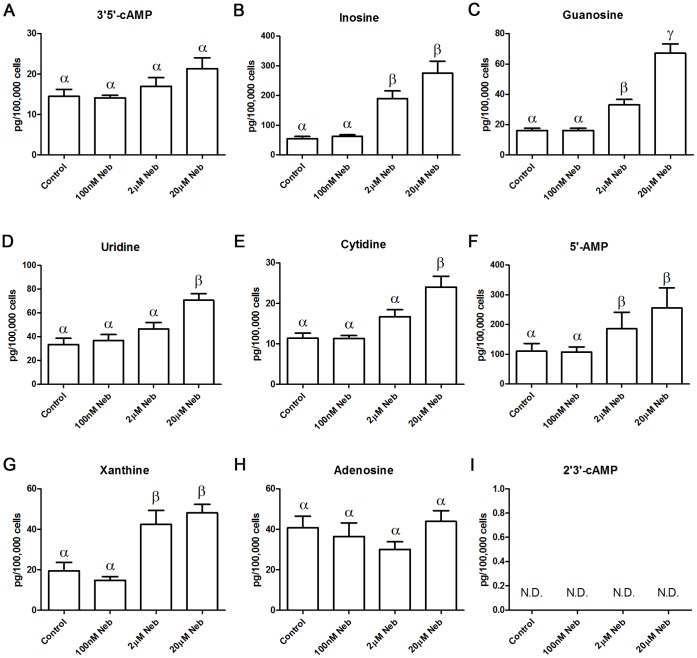
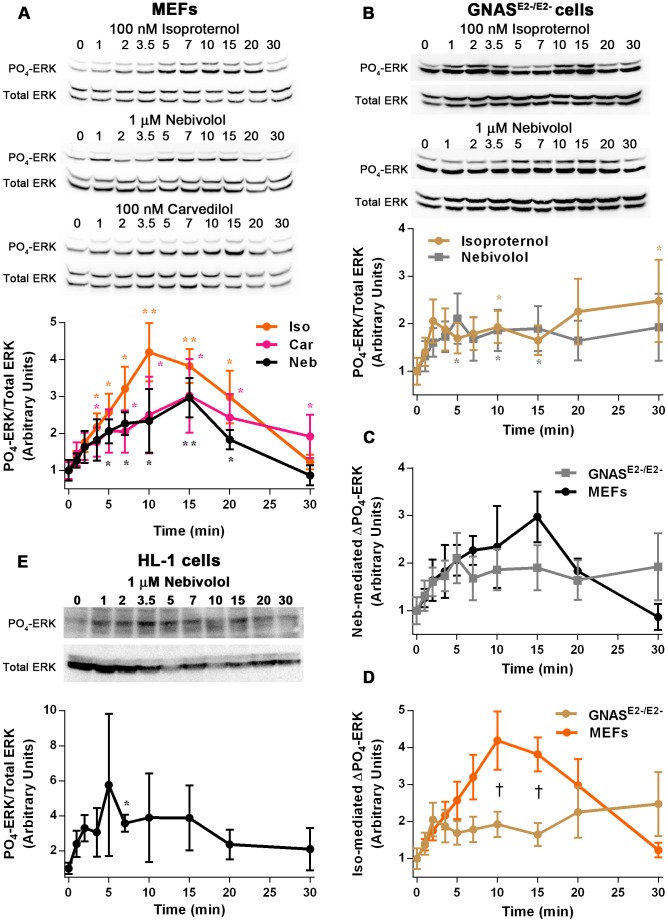
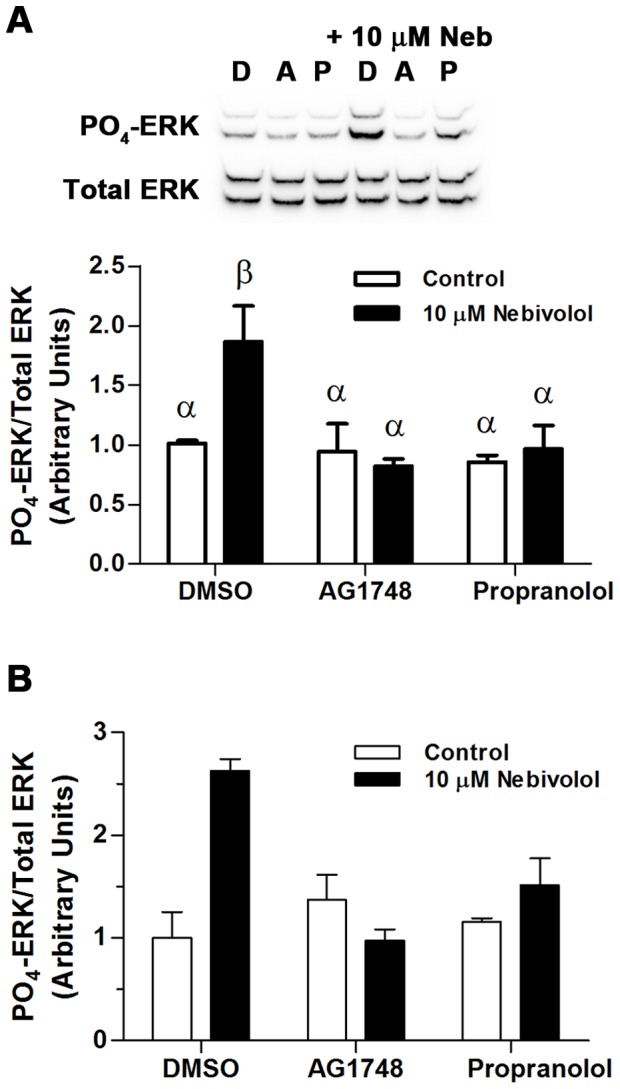
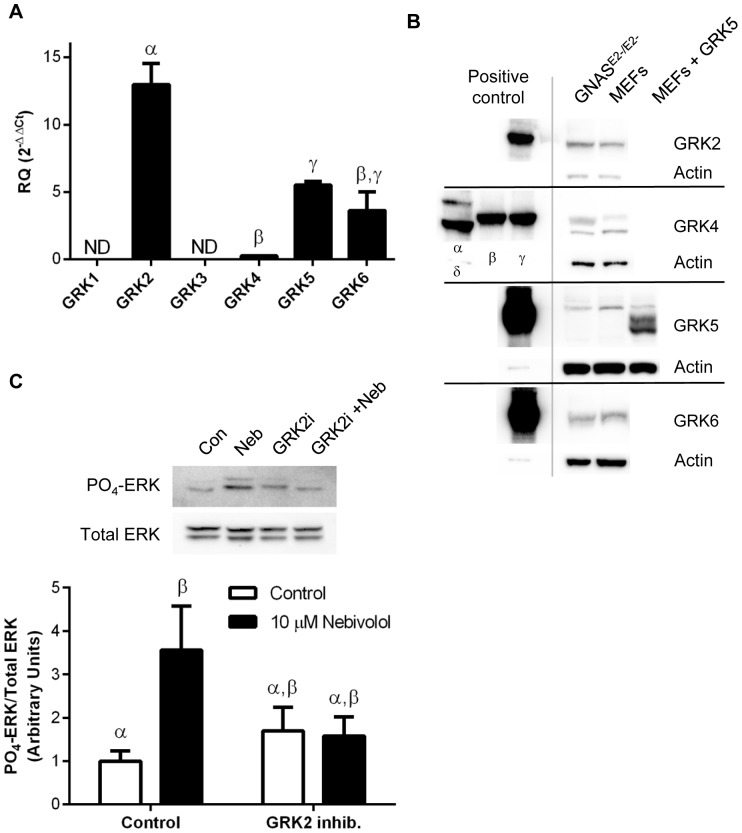
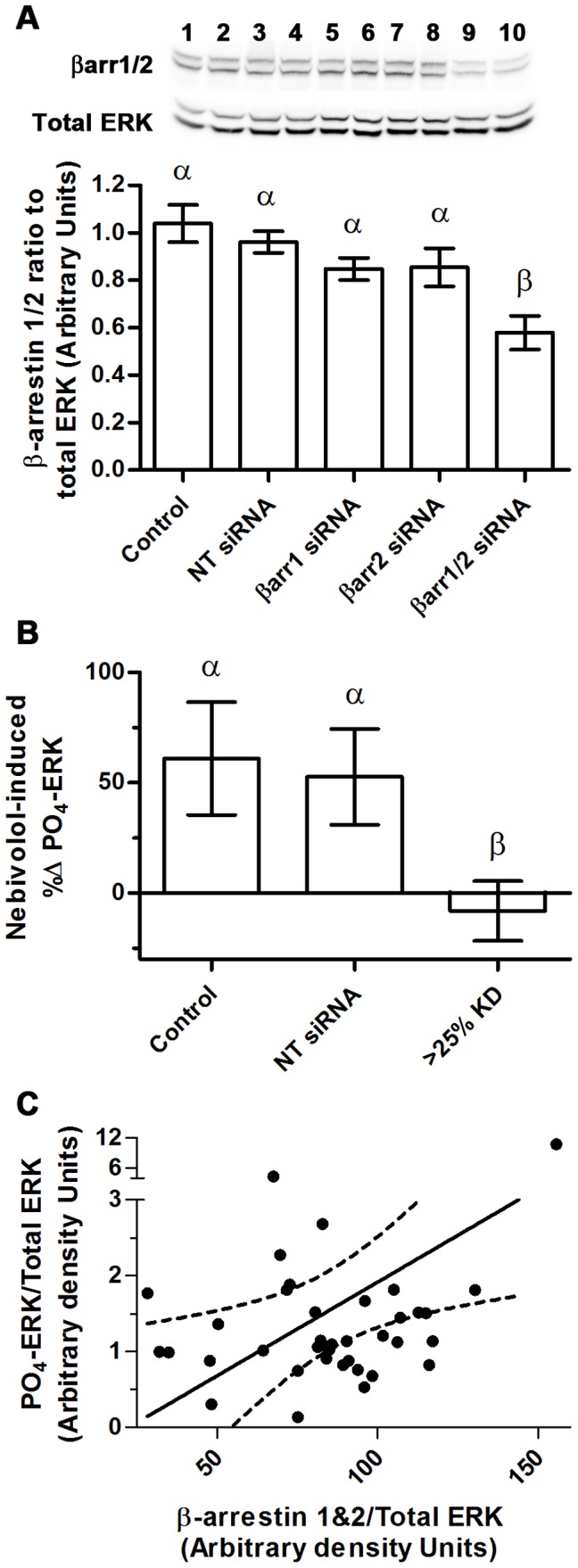
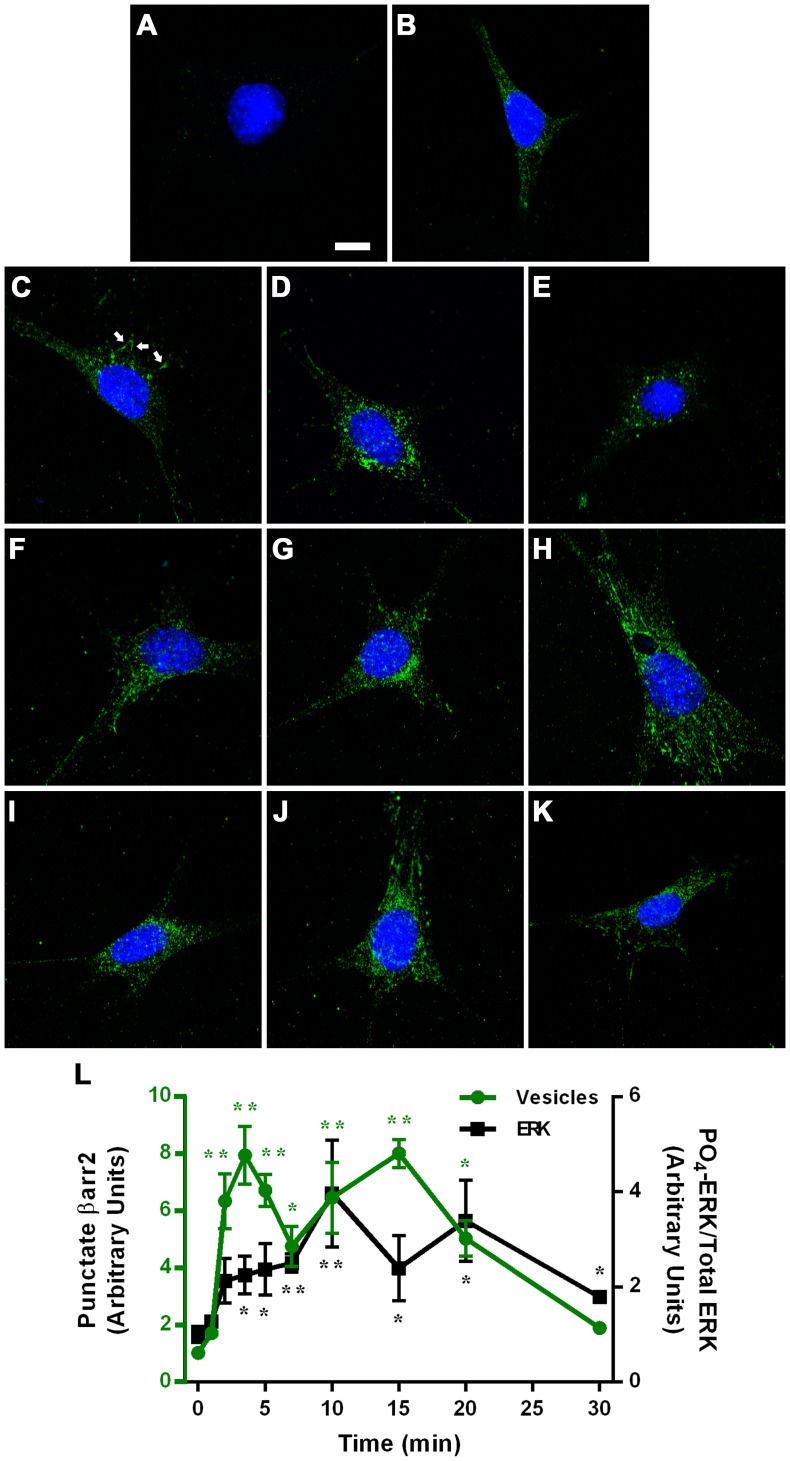
Nebivolol, a third generation β-adrenoceptor (β-AR) antagonist (β-blocker), causes vasodilation by inducing nitric oxide (NO) production. The mechanism via which nebivolol induces NO production remains unknown, resulting in the genesis of much of the controversy regarding the pharmacological action of nebivolol. Carvedilol is another β-blocker that induces NO production. A prominent pharmacological mechanism of carvedilol is biased agonism that is independent of Gαs and involves G protein-coupled receptor kinase (GRK)/β-arrestin signaling with downstream activation of the epidermal growth factor receptor (EGFR) and extracellular signal-regulated kinase (ERK). Due to the pharmacological similarities between nebivolol and carvedilol, we hypothesized that nebivolol is also a GRK/β-arrestin biased agonist. We tested this hypothesis utilizing mouse embryonic fibroblasts (MEFs) that solely express β2-ARs, and HL-1 cardiac myocytes that express β1- and β2-ARs and no detectable β3-ARs. We confirmed previous reports that nebivolol does not significantly alter cAMP levels and thus is not a classical agonist. Moreover, in both cell types, nebivolol induced rapid internalization of β-ARs indicating that nebivolol is also not a classical β-blocker. Furthermore, nebivolol treatment resulted in a time-dependent phosphorylation of ERK that was indistinguishable from carvedilol and similar in duration, but not amplitude, to isoproterenol. Nebivolol-mediated phosphorylation of ERK was sensitive to propranolol (non-selective β-AR-blocker), AG1478 (EGFR inhibitor), indicating that the signaling emanates from β-ARs and involves the EGFR. Furthermore, in MEFs, nebivolol-mediated phosphorylation of ERK was sensitive to pharmacological inhibition of GRK2 as well as siRNA knockdown of β-arrestin 1/2. Additionally, nebivolol induced redistribution of β-arrestin 2 from a diffuse staining pattern into more intense punctate spots. We conclude that nebivolol is a β2-AR, and likely β1-AR, GRK/β-arrestin biased agonist, which suggests that some of the unique clinically beneficial effects of nebivolol may be due to biased agonism at β1- and/or β2-ARs.
Conflict of interest statement
Figures
References
-
- Van de Water A, Janssens W, Van Neuten J, Xhonneux R, De Cree J, et al. (1988) Pharmacological and hemodynamic profile of nebivolol, a chemically novel, potent, and selective beta 1-adrenergic antagonist. J Cardiovasc Pharmacol 11: 552–563. - PubMed
-
- Cockcroft JR, Chowienczyk PJ, Brett SE, Chen CP, Dupont AG, et al. (1995) Nebivolol vasodilates human forearm vasculature: evidence for an L-arginine/NO-dependent mechanism. J Pharmacol Exp Ther 274: 1067–1071. - PubMed
-
- Feng MG, Prieto MC, Navar LG (2012) Nebivolol induced vasodilation of renal afferent arterioles involves beta3 adrenergic receptor and nitric oxide synthase activation. Am J Physiol Renal Physiol. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
