

A systematic review and meta-analysis on pulmonary resections by robotic video-assisted thoracic surgery
- PMID: 23977457
- PMCID: PMC3741728
- DOI: 10.3978/j.issn.2225-319X.2012.04.03
A systematic review and meta-analysis on pulmonary resections by robotic video-assisted thoracic surgery
Abstract
Background: Pulmonary resection by robotic video-assisted thoracic surgery (RVATS) has been performed for selected patients in specialized centers over the past decade. Despite encouraging results from case-series reports, there remains a lack of robust clinical evidence for this relatively novel surgical technique. The present systematic review aimed to assess the short- and long-term safety and efficacy of RVATS.
Methods: Nine relevant and updated studies were identified from 12 institutions using five electronic databases. Endpoints included perioperative morbidity and mortality, conversion rate, operative time, length of hospitalization, intraoperative blood loss, duration of chest drainage, recurrence rate and long-term survival. In addition, cost analyses and quality of life assessments were also systematically evaluated. Comparative outcomes were meta-analyzed when data were available.
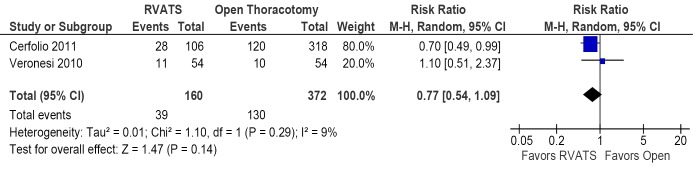
Results: All institutions used the same master-slave robotic system (da Vinci, Intuitive Surgical, Sunnyvale, California) and most patients underwent lobectomies for early-stage non-small cell lung cancers. Perioperative mortality rates for patients who underwent pulmonary resection by RVATS ranged from 0-3.8%, whilst overall morbidity rates ranged from 10-39%. Two propensity-score analyses compared patients with malignant disease who underwent pulmonary resection by RVATS or thoracotomy, and a meta-analysis was performed to identify a trend towards fewer complications after RVATS. In addition, one cost analysis and one quality of life study reported improved outcomes for RVATS when compared to open thoracotomy.
Conclusions: Results of the present systematic review suggest that RVATS is feasible and can be performed safely for selected patients in specialized centers. Perioperative outcomes including postoperative complications were similar to historical accounts of conventional VATS. A steep learning curve for RVATS was identified in a number of institutional reports, which was most evident in the first 20 cases. Future studies should aim to present data with longer follow-up, clearly defined surgical outcomes, and through an intention-to-treat analysis.
Keywords: Robotics; meta-analysis; minimally invasive surgery; systematic review; video-assisted thoracic surgery.
Figures
References
-
- Walker WS, Carnochan FM, Pugh GC. Thoracoscopic pulmonary lobectomy. Early operative experience and preliminary clinical results. J Thorac Cardiovasc Surg 1993;106:1111-7 - PubMed
-
- Kirby TJ, Rice TW. Thoracoscopic lobectomy. Ann Thorac Surg 1993;56:784-6 - PubMed
-
- Yan TD, Black D, Bannon PG, et al. Systematic review and meta-analysis of randomized and nonrandomized trials on safety and efficacy of video-assisted thoracic surgery lobectomy for early-stage non-small-cell lung cancer. J Clin Oncol 2009;27:2553-62 - PubMed
-
- Ashton RC, Jr, Connery CP, Swistel DG, et al. Robot-assisted lobectomy. J Thorac Cardiovasc Surg 2003;126:292-3 - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous