

Consensus on hypothermia in aortic arch surgery
- PMID: 23977577
- PMCID: PMC3741830
- DOI: 10.3978/j.issn.2225-319X.2013.03.03
Consensus on hypothermia in aortic arch surgery
Abstract
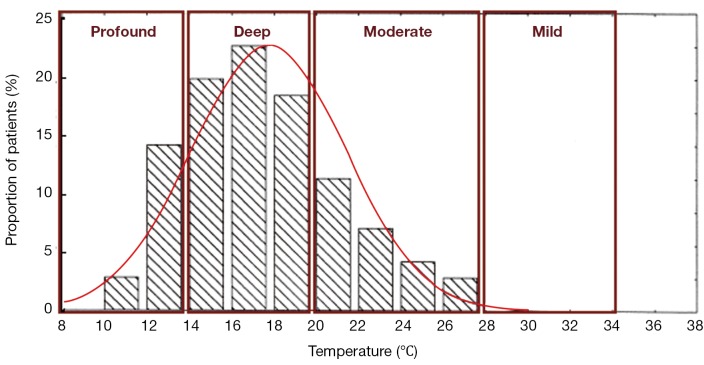
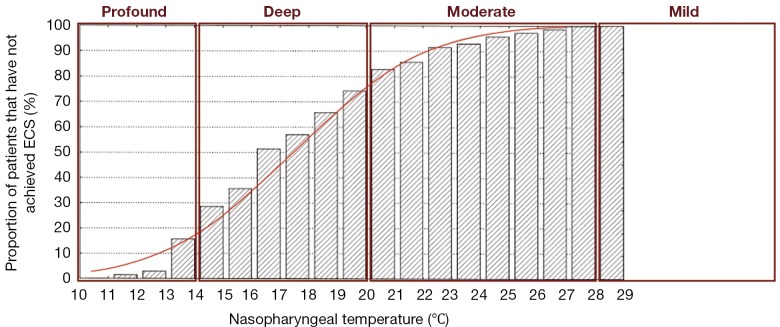
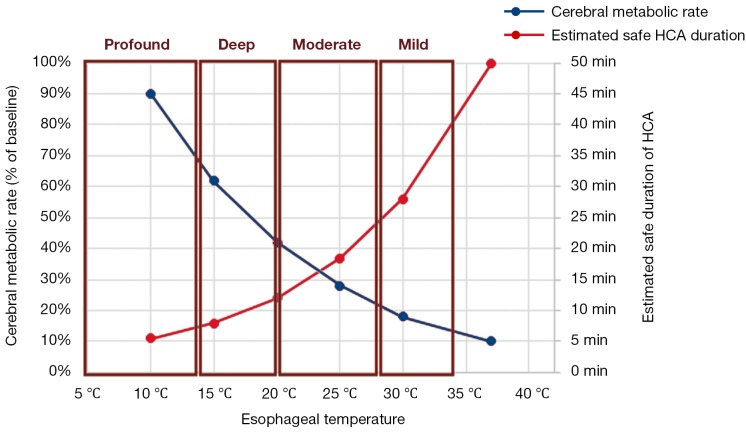
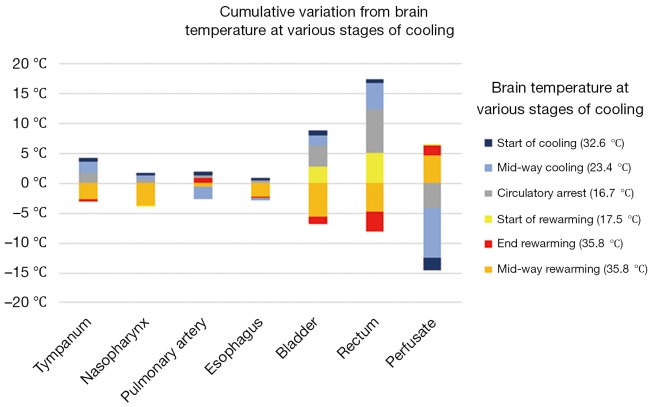
Considered a standard part of aortic arch surgery, hypothermia can sufficiently reduce cerebral metabolic demand to permit reasonable periods of circulatory arrest. Yet despite its ubiquitous application and critical importance, temperature classification in hypothermic circulatory arrest is still without clear definition. The following Consensus from experts in high-volume aortic institutions defines 'profound', 'deep', 'moderate', and 'mild' hypothermia and recommends standardized monitoring sites, so as to facilitate more consistent reporting and robust analysis.
Keywords: Aortic arch surgery; cerebral protection; consensus statement; hypothermic circulatory arrest.
Figures
References
-
- Kamiya H, Hagl C, Kropivnitskaya I, et al. The safety of moderate hypothermic lower body circulatory arrest with selective cerebral perfusion: a propensity score analysis. J Thorac Cardiovasc Surg 2007;133:501-9 - PubMed
-
- Stecker MM, Cheung AT, Pochettino A, et al. Deep hypothermic circulatory arrest: I. Effects of cooling on electroencephalogram and evoked potentials. Ann Thorac Surg 2001;71:14-21 - PubMed
-
- McCullough JN, Zhang N, Reich DL, et al. Cerebral metabolic suppression during hypothermic circulatory arrest in humans. Ann Thorac Surg 1999;67:1895-9; discussion 1919-21. - PubMed
-
- Svensson LG, Crawford ES, Hess KR, et al. Deep hypothermia with circulatory arrest. Determinants of stroke and early mortality in 656 patients. J Thorac Cardiovasc Surg 1993;106:19-28; discussion 28-31 - PubMed
LinkOut - more resources
Full Text Sources
Medical