

Type I and Type II hybrid aortic arch replacement: postoperative and mid-term outcome analysis
- PMID: 23977595
- PMCID: PMC3741847
- DOI: 10.3978/j.issn.2225-319X.2013.05.09
Type I and Type II hybrid aortic arch replacement: postoperative and mid-term outcome analysis
Abstract
Background: Hybrid aortic arch replacement has emerged as a safe treatment modality for arch aneurysms, especially in patients of old age and with greater comorbid burden. We assessed our institutional outcomes in patients undergoing Types I and II hybrid aortic arch replacement.
Methods: From 2005 to 2012, 685 patients underwent thoracic endovascular repair (TEVAR), of whom 104 had hybrid arch repair (open + endovascular approach). 47 of these patients had treatment for aortic arch aneurysm ± proximal ascending aortic aneurysm. The hybrid repair entailed aortic arch vessel debranching and concomitant/delayed antegrade ± retrograde TEVAR stent grafting of the arch. Type III patients were excluded from the analysis. Data was prospectively maintained.
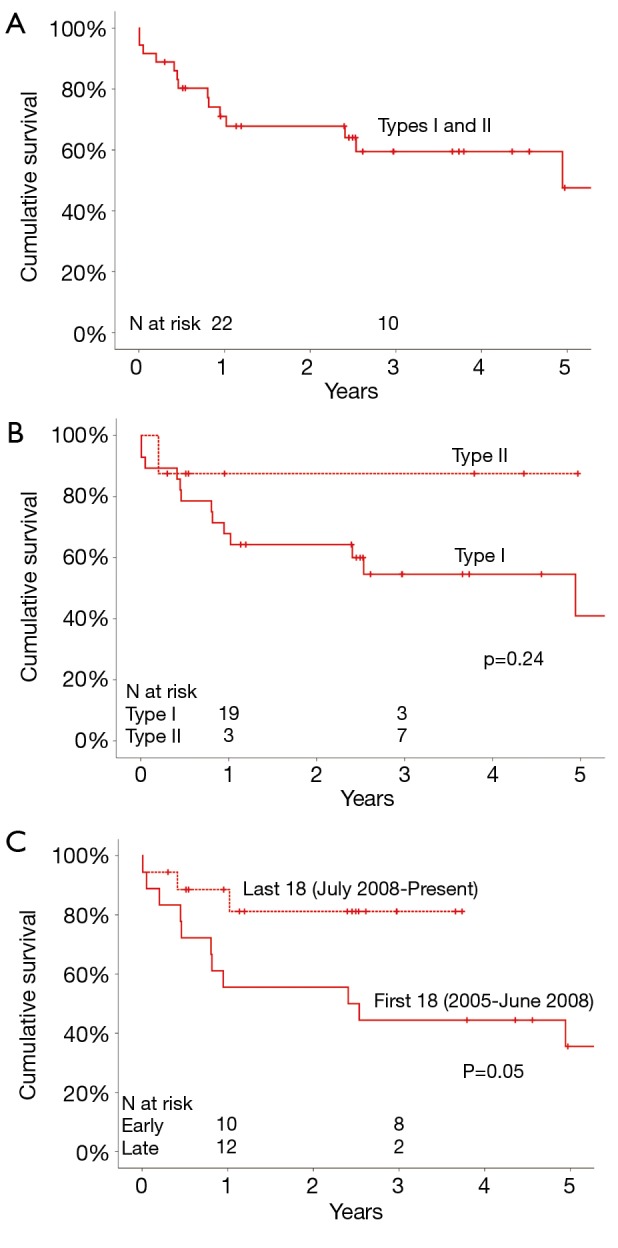
Results: 28 patients had Type I repair, 8 had Type II repair, and 11 had Type III repair. Mean age was 71±8 years. Primary aortic pathology was aneurysm (81%), followed by chronic arch dissection (11%). 14% of patients required reoperative cardiac surgery. Stent graft deployment rate was 100% after arch vessel debranching. Postoperative endoleak rate was zero. Average cardiopulmonary bypass time was 215±64 minutes, with crossclamp time of 70±55 minutes, and circulatory arrest time of 50±17 minutes. Paraplegia rate was 5.5% (n=2), with stroke rate of 8% (n=3) and renal failure rate of 3% (n=1) requiring hemodialysis. In-hospital mortality was 8% (n=3). Mean length of stay was 17.2±14 days. Median follow-up was 30±21 months. Freedom from all-cause mortality was 71%, 60%, and 48% at 1, 3, and 5 years respectively. Aortic reoperation rate was 2.7% (n=1). No patient had Type I or III endoleak at follow-up. Freedom from mortality was improved in cases performed more recently (July 2008 to 2012) than during our early experience (2005 to June 2008) (81% versus 44% at 3 years, P=0.05).
Conclusions: Hybrid aortic arch replacement can be performed with good postoperative and midterm results in a cohort of old patients with significant comorbidity. With greater experience, early and midterm outcomes continue to improve. The hybrid arch technique may represent a technical advancement in the field of aortic arch surgery.
Keywords: Hybrid aortic arch replacement; midterm outcome; postoperative outcome; thoracic endovascular repair (TEVAR).
Figures

References
-
- Svensson LG, Kim KH, Blackstone EH, et al. Elephant trunk procedure: newer indications and uses. Ann Thorac Surg 2004;78:109-16; discussion 109-16 - PubMed
-
- Svensson LG, Crawford ES, Hess KR, et al. Deep hypothermia with circulatory arrest. Determinants of stroke and early mortality in 656 patients. J Thorac Cardiovasc Surg 1993;106:19-28; discussion 28-31 - PubMed
-
- Sundt TM, 3rd, Orszulak TA, Cook DJ, et al. Improving results of open arch replacement. Ann Thorac Surg 2008;86:787-96; discussion 787-96 - PubMed
-
- Zeeshan A, Woo EY, Bavaria JE, et al. Thoracic endovascular aortic repair for acute complicated type B aortic dissection: superiority relative to conventional open surgical and medical therapy. J Thorac Cardiovasc Surg 2010;140:S109-15; discussion S142-S146. - PubMed
-
- Frigiola A, Ranucci M, Carlucci C, et al. The Ross procedure in adults: long-term follow-up and echocardiographic changes leading to pulmonary autograft reoperation. Ann Thorac Surg 2008;86:482-9 - PubMed
LinkOut - more resources
Full Text Sources