

Microtomographic analysis of lower urinary tract obstruction
- PMID: 23977847
- PMCID: PMC3965709
- DOI: 10.2350/13-08-1359-OA.1
Microtomographic analysis of lower urinary tract obstruction
Abstract
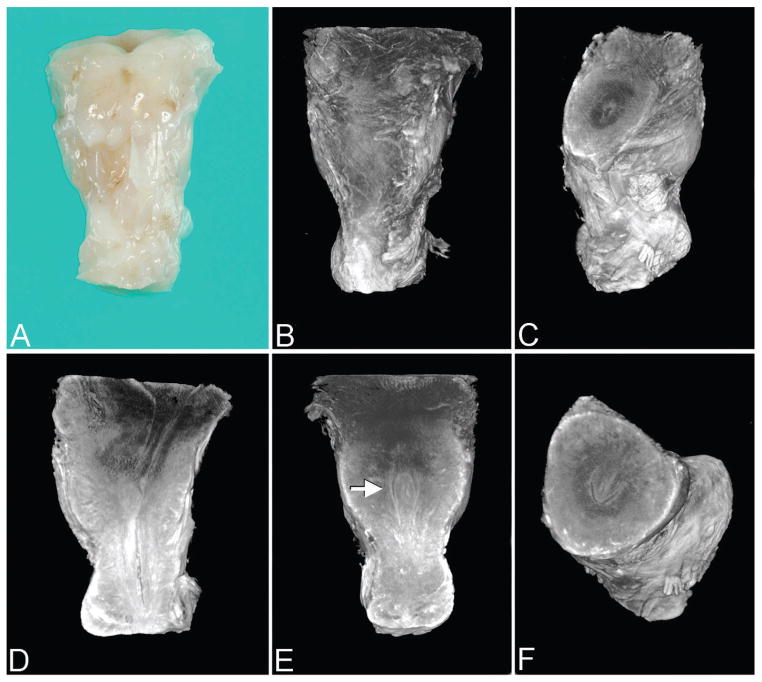
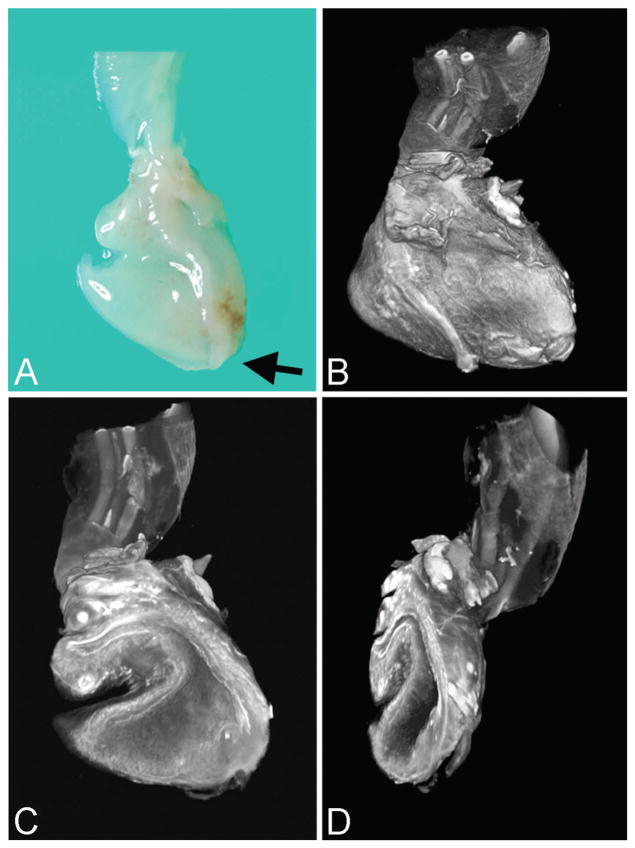
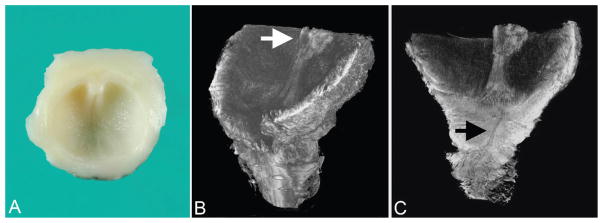
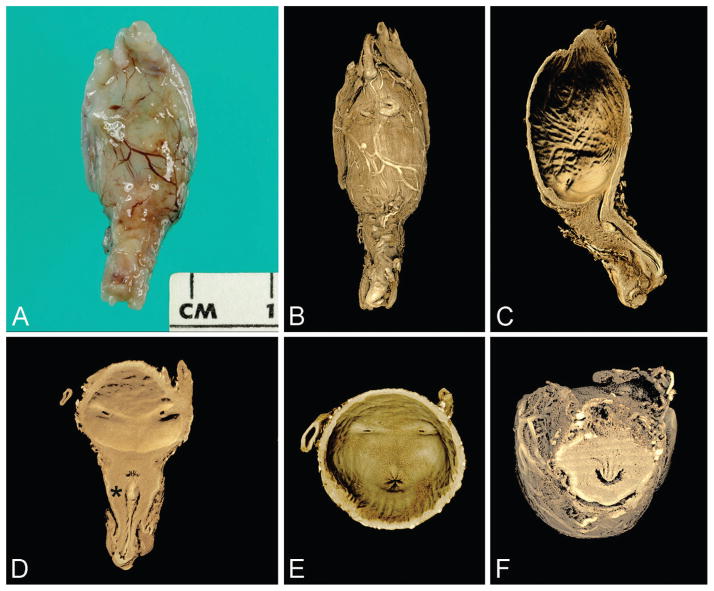
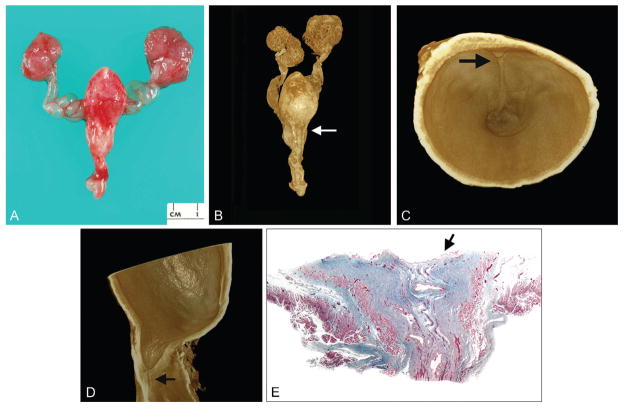
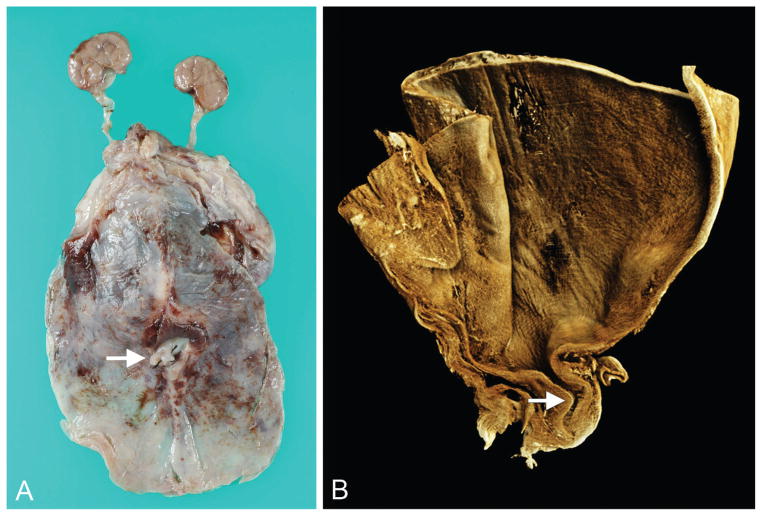
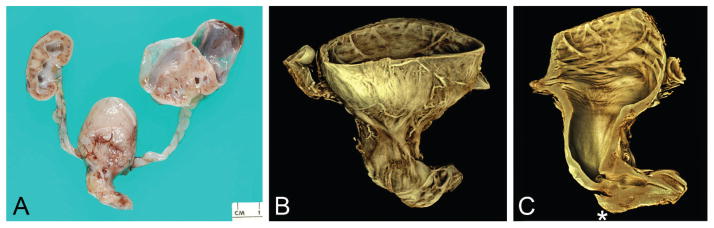
Prenatal obstruction of the lower urinary tract may result in megacystis, with subsequent development of hydroureter, hydronephrosis, and renal damage. Oligo- or anhydramnios, pulmonary hypoplasia, and prune belly syndrome are lethal consequences. Causes and mechanisms responsible for obstruction remain unclear but might be clarified by anatomic study at autopsy. To this end, we employed 2 methods of tomographic imaging-optical projection tomography and contrast-enhanced microCT scanning-to elucidate the anatomy of the intact urinary bladder and urethra in 10 male fetuses with lower urinary tract obstruction. Images were compared with those from 9 age-matched controls. Three-dimensional images, rotated and sectioned digitally in multiple planes, permitted thorough examination while preserving specimens for later study. Both external and internal features of the bladder and urethra were demonstrated; small structures (ie, urethral crest, verumontanum, prostatic utricle, ejaculatory ducts) were seen in detail. Types of obstruction consisted of urethral atresia (n = 5), severe urethral stenosis (n = 2), urethral diaphragm (n = 2), or physical kinking (n = 1); classic (Young type I) posterior urethral valves were not encountered. Traditional light microscopy was then used to verify tomographic findings. The prostate gland was hypoplastic or absent in all cases; in 1, prostatic tissue was displaced inferior to the verumontanum. Findings support previous views that dissection may produce valve-like artifacts (eg, bisection of an obstructing diaphragm) and that deformation of an otherwise normal urethra may result in megacystis. The designation "posterior urethral valves" should not be used as a generic expression of urethral obstruction unless actual valves are demonstrated.
Figures
References
-
- Young HH, Frontz WA, Baldwin JC. Congenital obstruction of the posterior urethra. J Urol. 1919;3:289–365. - PubMed
-
- Stevens FD. Anus and Genito-Urinary Tracts. Edinburgh: E. & S. Livingstone Ltd; 1963. Congenital Malformations of the Rectum.
-
- Schreuder MF, van der Horst HJ, Bökenkamp A, et al. Posterior urethral valves in three siblings: a case report and review of the literature. Birth Defects Res A Clin Mol Teratol. 2008;82:232–235. - PubMed
-
- Siebert JR, Walker MPR. Familial recurrence of urethral stenosis/atresia. Birth Defects Res A. 2009;85:715–719. - PubMed
-
- Kajbafzadeh A. Congenital urethral anomalies in boys. Part I: posterior urethral valves. Urol J. 2005;2:59–78. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
