

Differential treatment of hypertension by primary care providers and hypertension specialists in a barber-based intervention trial to control hypertension in Black men
- PMID: 23978276
- PMCID: PMC3800500
- DOI: 10.1016/j.amjcard.2013.07.004
Differential treatment of hypertension by primary care providers and hypertension specialists in a barber-based intervention trial to control hypertension in Black men
Abstract
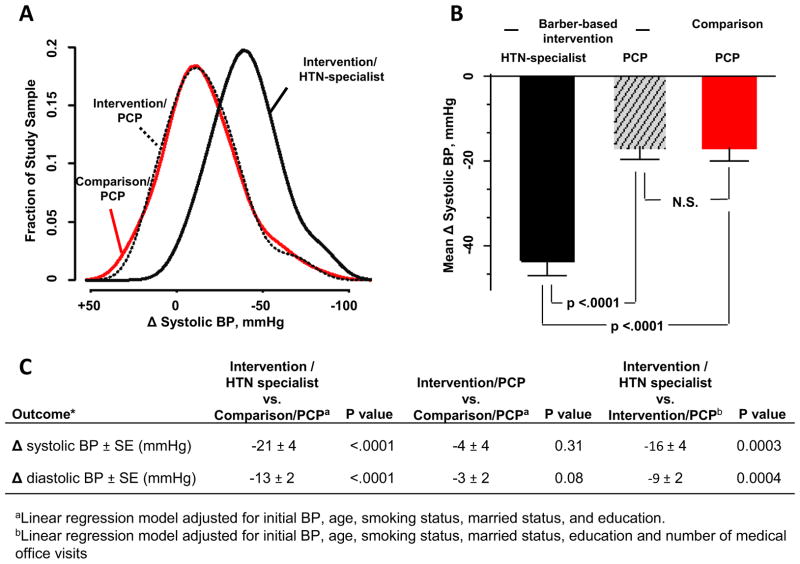
Black men have less physician contact than other groups and thus lower rates of hypertension treatment and control. In the Barber-Assisted Reduction in Blood Pressure among Ethnic Residents trial, hypertension control in 8 active-intervention barbershops where barbers offered blood pressure (BP) checks with haircuts and motivated black male patrons with high BP to seek provider follow-up showed a small improvement over that in 7 comparison shops where patrons received hypertension pamphlets but not barber-BP checks. Undertreatment of hypertension, which is common in primary care, may have impacted the outcomes. Thus, in patrons with a baseline systolic BP of ≥140 mm Hg and 10-month follow-up including BP and medication data, we performed post hoc comparison of systolic BP reduction between comparison-arm patrons (n = 68) treated by primary care providers (PCPs) with (1) intervention-arm patrons (n = 37) treated by PCPs or (2) intervention-arm patrons (n = 33) who lacked access to PCPs and were treated by hypertension specialist physicians serving as safety net providers. The latter group had higher baseline systolic BP than the others (162 ± 3 vs 155 ± 2 and 154 ± 2 mm Hg, respectively, p <0.01). After adjustment for baseline systolic BP and other covariates, systolic BP reduction was 21 ± 4 mm Hg greater than in the comparison group (p <0.0001), when barbers referred patrons to hypertension specialists but was no different when they referred to PCPs (4 ± 4 mm Hg, p = 0.31). Specialist-treated patrons received more BP medication and different classes of medication than PCP-treated patrons. In conclusion, the barber-based intervention-if connected directly to specialty-level medical care-could have a large public health impact on hypertensive disease in black men.
Trial registration: ClinicalTrials.gov NCT00325533.
Copyright © 2013 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS, Franco S, Fullerton HJ, Gillespie C, Hailpern SM, Heit JA, Howard VJ, Huffman MD, Kissela BM, Kittner SJ, Lackland DT, Lichtman JH, Lisabeth LD, Magid D, Marcus GM, Marelli A, Matchar DB, McGuire DK, Mohler ER, Moy CS, Mussolino ME, Nichol G, Paynter NP, Schreiner PJ, Sorlie PD, Stein J, Turan TN, Virani SS, Wong ND, Woo D, Turner MB American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Executive summary: heart disease and stroke statistics--2013 update: a report from the American Heart Association. Circulation. 2013;127:143–152. - PubMed
-
- Guo F, He D, Zhang W, Walton RG. Trends in prevalence, awareness, management, and control of hypertension among United States adults, 1999 to 2010. J Am Coll Cardiol. 2012;60:599–606. - PubMed
-
- Wright JT, Jr, Dunn JK, Cutler JA, Davis BR, Cushman WC, Ford CE, Haywood LJ, Leenen FH, Margolis KL, Papademetriou V, Probstfield JL, Whelton PK, Habib GB ALLHAT Collaborative Research Group. Outcomes in hypertensive black and nonblack patients treated with chlorthalidone, amlodipine, and lisinopril. JAMA. 2005;293:1595–1608. - PubMed
-
- Victor RG, Leonard D, Hess P, Bhat DG, Jones J, Vaeth PA, Ravenell J, Freeman A, Wilson RP, Haley RW. Factors associated with hypertension awareness, treatment, and control in Dallas County, Texas. Arch Intern Med. 2008;168:1285–1293. - PubMed
-
- Hyman DJ, Pavlik VN. Characteristics of patients with uncontrolled hypertension in the United States. N Engl J Med. 2001;345:479–486. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
