

The John Insall Award: A minimum 10-year outcome study of autologous chondrocyte implantation
- PMID: 23979923
- PMCID: PMC3889462
- DOI: 10.1007/s11999-013-3146-9
The John Insall Award: A minimum 10-year outcome study of autologous chondrocyte implantation
Abstract
Background: Autologous chondrocyte implantation (ACI) has demonstrated good and excellent results in over 75% of patients up to 10 years after surgery. Reports of longer-term outcomes, however, remain limited.
Questions/purposes: The purposes of this study were to describe the (1) survivorship of ACI grafts; (2) the long-term functional outcomes using validated scoring tools after ACI; and (3) to provide an analysis of potential predictors for failure.
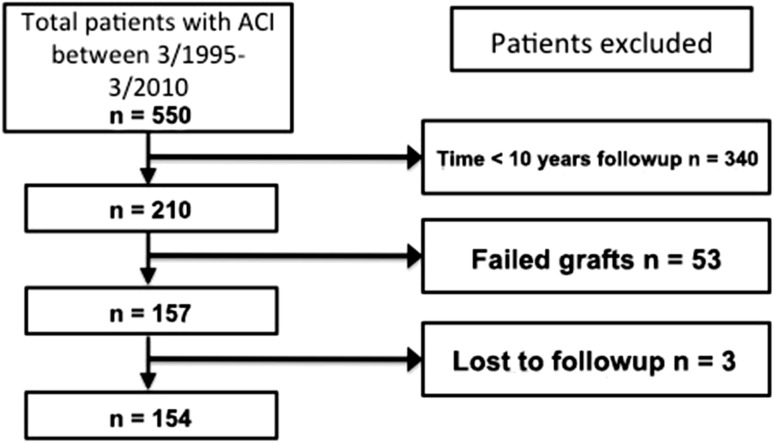
Methods: Two hundred ten patients treated with ACI were followed for more than 10 years. Indications for the procedure included symptomatic cartilage defects in all compartments of the knee unresponsive to nonoperative measures. Mean age at surgery was 36 ± 9 years; mean defect size measured 8.4 ± 5.5 cm(2). Outcome scores were prospectively collected pre- and postoperatively at the last followup.
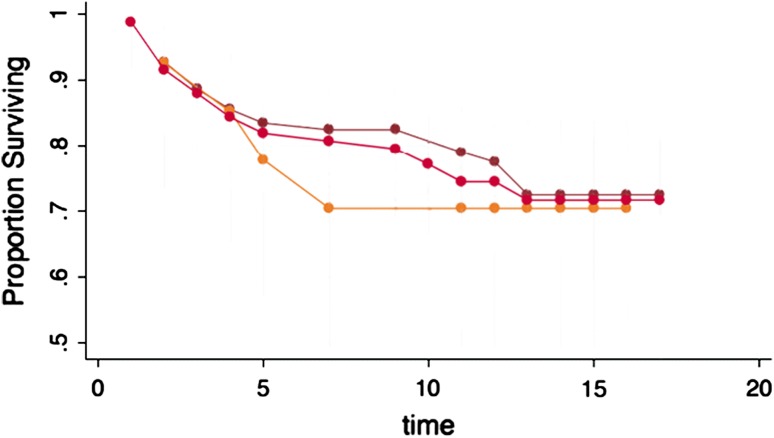
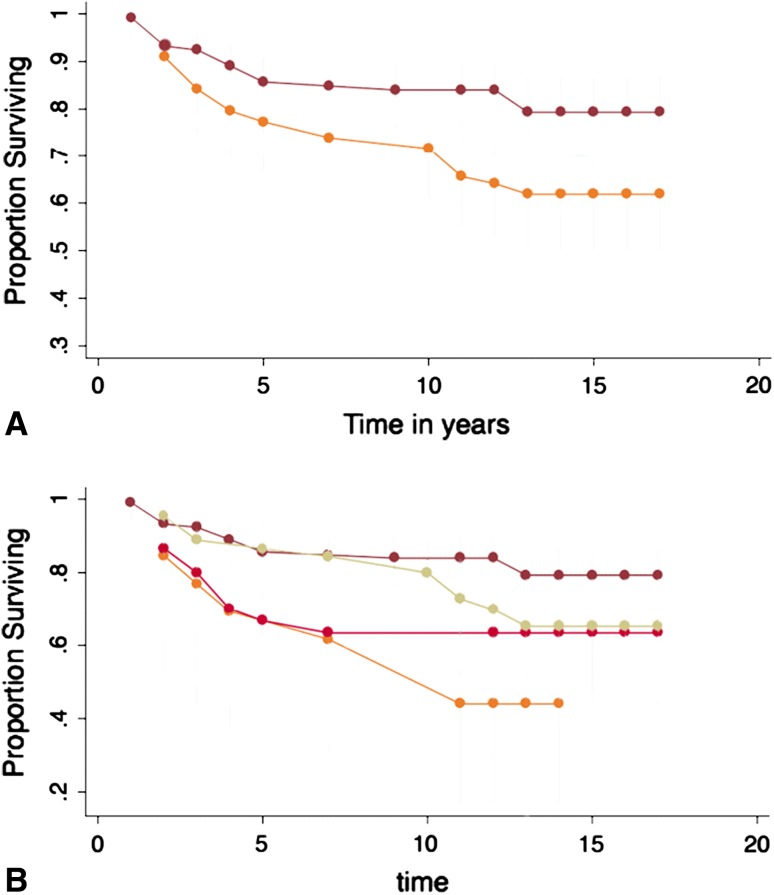
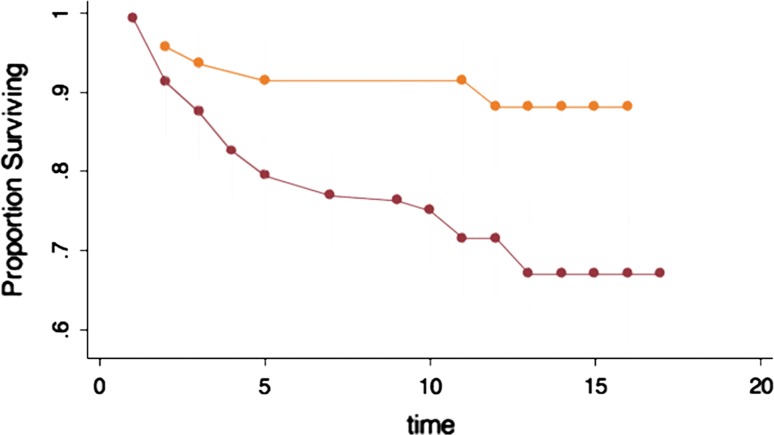
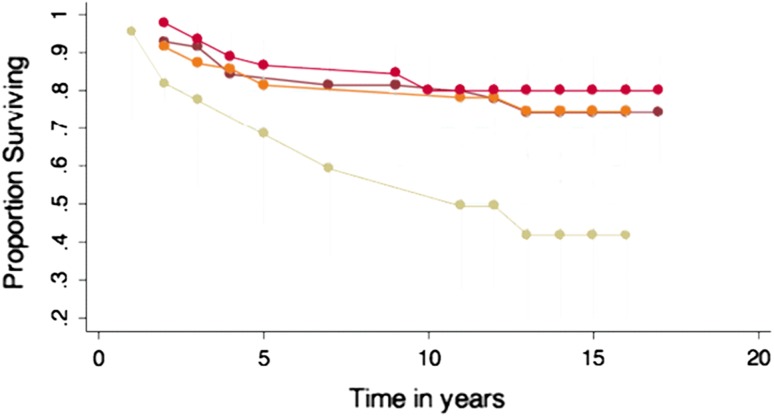
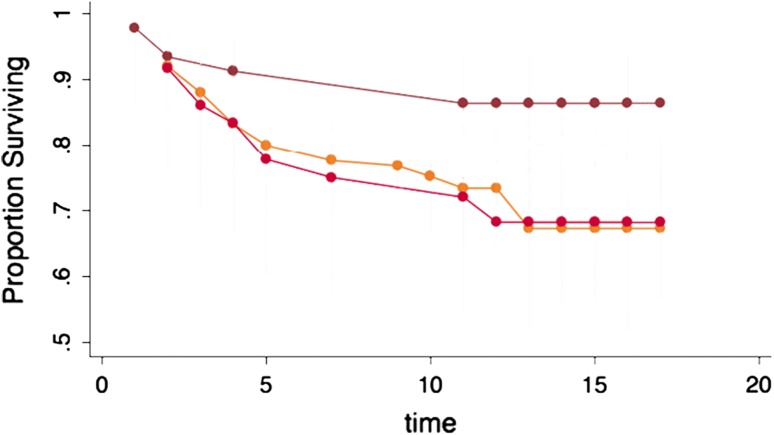
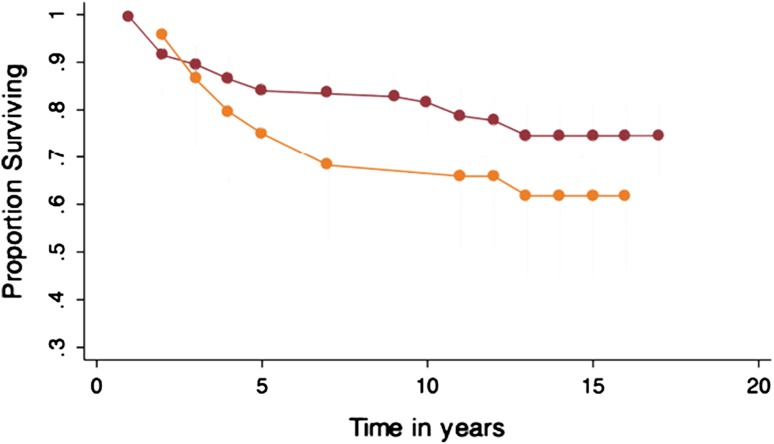
Results: At a mean of 12 ± 2 years followup, 53 of 210 patients (25%) had at least one failed ACI graft. Nineteen of these patients went on to arthroplasty, 27 patients were salvaged with revision cartilage repair, and seven patients declined further treatment; three patients were lost to followup. The modified Cincinnati increased from 3.9 ± 1.5 to 6.4 ± 1.5, WOMAC improved from 39 ± 21 to 23 ± 16, Knee Society Score (KSS) knee score rose from 54 ± 18 to 79 ± 19, and KSS function from 65 ± 23 to 78 ± 17 (all p < 0.0001). The Physical Component of the SF-36 score increased from 33 ± 14 to 49 ± 18, whereas the Mental Component improved from 46 ± 14 to 52 ± 15 (both p < 0.001). Survivorship was higher in patients with complex versus salvage-type lesions (p = 0.03) with primary ACI versus ACI after prior marrow stimulation (p = 0.004) and with concomitant high tibial osteotomy (HTO) versus no HTO (p = 0.01).
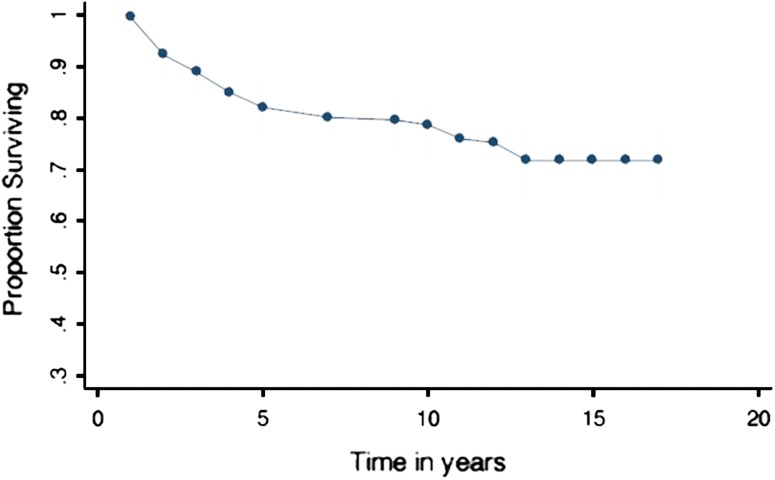
Conclusions: ACI provided durable outcomes with a survivorship of 71% at 10 years and improved function in 75% of patients with symptomatic cartilage defects of the knee at a minimum of 10 years after surgery. A history of prior marrow stimulation as well as the treatment of very large defects was associated with an increased risk of failure.
Figures
References
-
- Angst F, Aeschlimann A, Michel BA, Stucki G. Minimal clinically important rehabilitation effects in patients with osteoarthritis of the lower extremities. J Rheumatol. 2002;29:131–138. - PubMed
-
- Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol. 1988;15:1833–1840. - PubMed
-
- Bitton R. The economic burden of osteoarthritis. Am J Manag Care. 2009;15:S230–S235. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
