

The effect of three or six years of denosumab exposure in women with postmenopausal osteoporosis: results from the FREEDOM extension
- PMID: 23979955
- PMCID: PMC4207950
- DOI: 10.1210/jc.2013-1597
The effect of three or six years of denosumab exposure in women with postmenopausal osteoporosis: results from the FREEDOM extension
Abstract
Context: The Fracture Reduction Evaluation of Denosumab in Osteoporosis Every 6 Months (FREEDOM) extension is evaluating the long-term efficacy and safety of denosumab for up to 10 years.
Objective: The objective of the study was to report results from the first 3 years of the extension, representing up to 6 years of denosumab exposure.
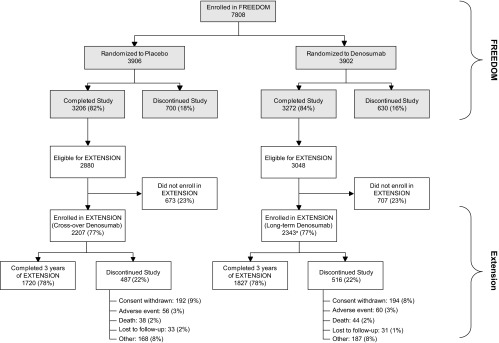
Design, setting, and participants: This was a multicenter, international, open-label study of 4550 women.
Intervention: Women from the FREEDOM denosumab group received 3 more years of denosumab for a total of 6 years (long-term) and women from the FREEDOM placebo group received 3 years of denosumab (crossover).
Main outcome measures: Bone turnover markers (BTMs), bone mineral density (BMD), fracture, and safety data are reported.
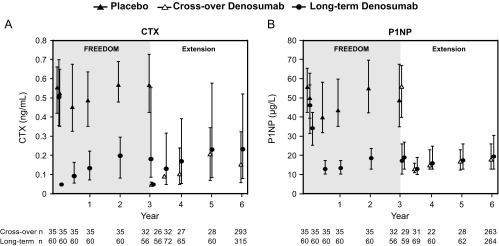
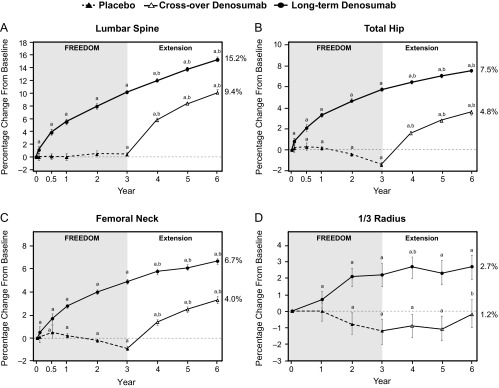
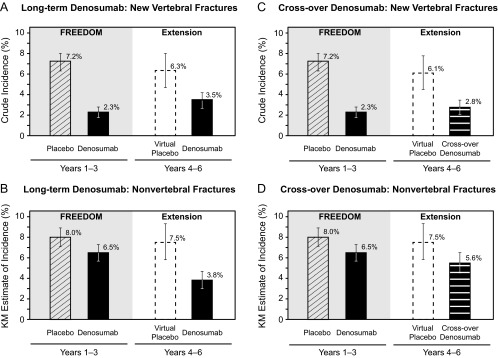
Results: Reductions in BTMs were maintained (long-term) or achieved rapidly (crossover) after denosumab administration. In the long-term group, BMD further increased for cumulative 6-year gains of 15.2% (lumbar spine) and 7.5% (total hip). During the first 3 years of denosumab treatment, the crossover group had significant gains in lumbar spine (9.4%) and total hip (4.8%) BMD, similar to the long-term group during the 3-year FREEDOM trial. In the long-term group, fracture incidences remained low and below the rates projected for a virtual placebo cohort. In the crossover group, 3-year incidences of new vertebral and nonvertebral fractures were similar to those of the FREEDOM denosumab group. Incidence rates of adverse events did not increase over time. Six participants had events of osteonecrosis of the jaw confirmed by adjudication. One participant had a fracture adjudicated as consistent with atypical femoral fracture.
Conclusion: Denosumab treatment for 6 years remained well tolerated, maintained reduced bone turnover, and continued to increase BMD. Fracture incidence remained low.
Trial registration: ClinicalTrials.gov NCT00523341.
Figures
References
-
- Kostenuik PJ. Osteoprotegerin and RANKL regulate bone resorption, density, geometry and strength. Curr Opin Pharmacol. 2005;5:618–625 - PubMed
-
- Boyle WJ, Simonet WS, Lacey DL. Osteoclast differentiation and activation. Nature. 2003;423:337–342 - PubMed
-
- Sambrook P, Cooper C. Osteoporosis. Lancet. 2006;367:2010–2018 - PubMed
-
- Bone Health and Osteoporosis. A Report of the Surgeon General. Bethesda, MD: US Department of Health and Human Services
-
- Seeman E, Delmas PD. Bone quality—the material and structural basis of bone strength and fragility. N Engl J Med. 2006;354:2250–2261 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
