

Identification of concurrent bacterial infection in adult patients with dengue
- PMID: 23980129
- PMCID: PMC3795118
- DOI: 10.4269/ajtmh.13-0197
Identification of concurrent bacterial infection in adult patients with dengue
Abstract
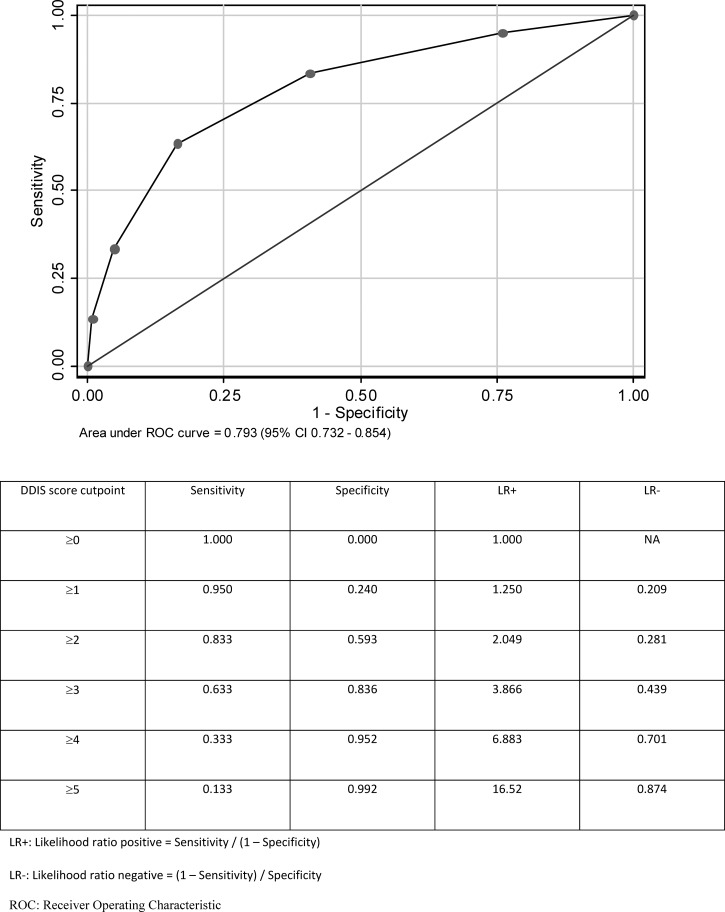
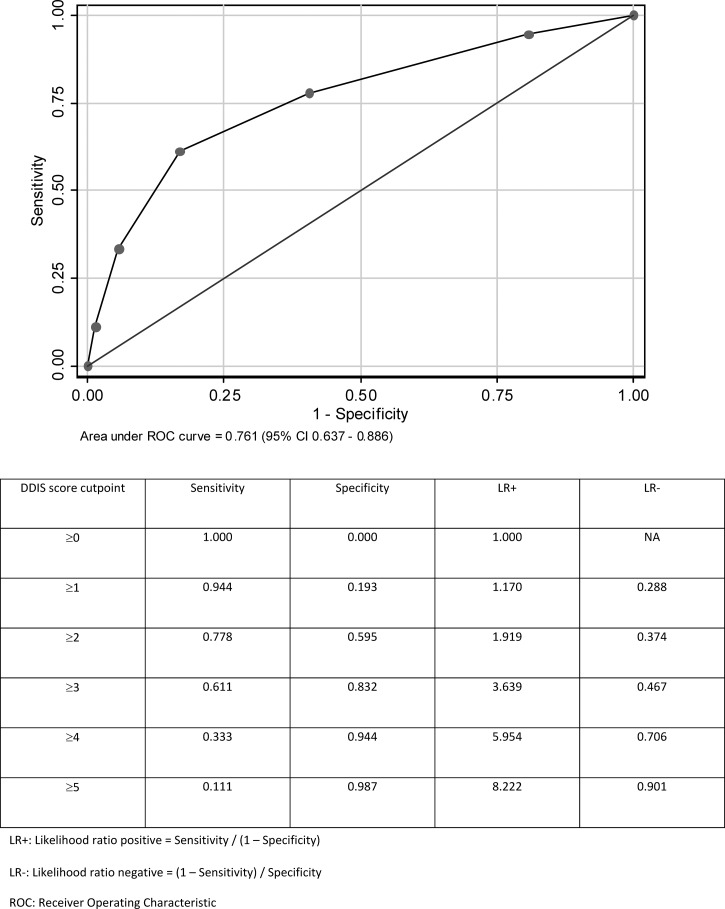
We aim to construct a diagnostic model for bacterial coinfection in dengue patients (Dengue Dual Infection Score [DDIS]); 2,065 adult dengue patients (mean age = 41.9 ± 17.2 years, 58.4% male, 83 patients with bacterial coinfection) seen at a university hospital from January of 2005 to February of 2010 were studied. The DDIS was created by assigning one point to each of five risk factors for bacterial coinfection: pulse rate ≥ 90 beats/minute, total white cell count ≥ 6 × 10(9)/L, hematocrit < 40%, serum sodium < 135 mmol/L, and serum urea ≥ 5 mmol/L. The DDIS identified bacterial coinfection (derivation set area under the curve = 0.793, 95% confidence interval = 0.732-0.854; validation set area under the curve = 0.761, 95% confidence interval = 0.637-0.886). A DDIS of ≥ 4 had a specificity of 94.4%, whereas a DDIS of ≥ 1 had a sensitivity of 94.4% for bacterial coinfection. The DDIS can help to select dengue patients for early bacterial cultures and empirical antibiotics.
Figures
References
-
- Wilder-Smith A, Schwartz E. Dengue in travelers. N Engl J Med. 2005;353:924–932. - PubMed
-
- Halstead SB. Dengue. Lancet. 2007;370:1644–1652. - PubMed
-
- Wilder-Smith A, Renhorn KE, Tissera H, Abu Bakar S, Alphey L, Kittayapong P, Lindsay S, Logan J, Hatz C, Reiter P, Rocklov J, Byass P, Louis VR, Tozan Y, Massad E, Tenorio A, Lagneau C, L'Ambert G, Brooks D, Wegerdt J, Gubler D. DengueTools: innovative tools and strategies for the surveillance and control of dengue. Glob Health Action. 2012;2012:5. - PMC - PubMed
-
- Rigau-Perez JG, Clark GG, Gubler DJ, Reiter P, Sanders EJ, Vorndam AV. Dengue and dengue haemorrhagic fever. Lancet. 1998;352:971–977. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
