

What is the origin of the arterial vascularization of the corpora cavernosa? A computer-assisted anatomic dissection study
- PMID: 23981086
- PMCID: PMC4399354
- DOI: 10.1111/joa.12094
What is the origin of the arterial vascularization of the corpora cavernosa? A computer-assisted anatomic dissection study
Abstract
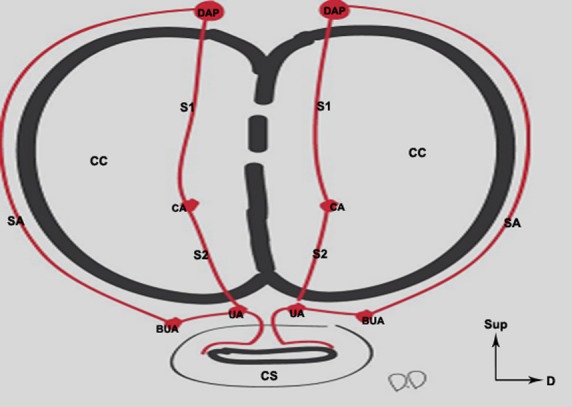
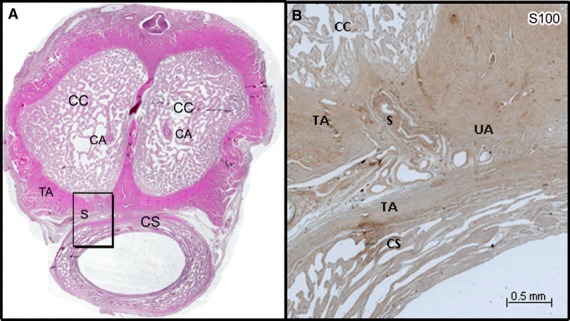
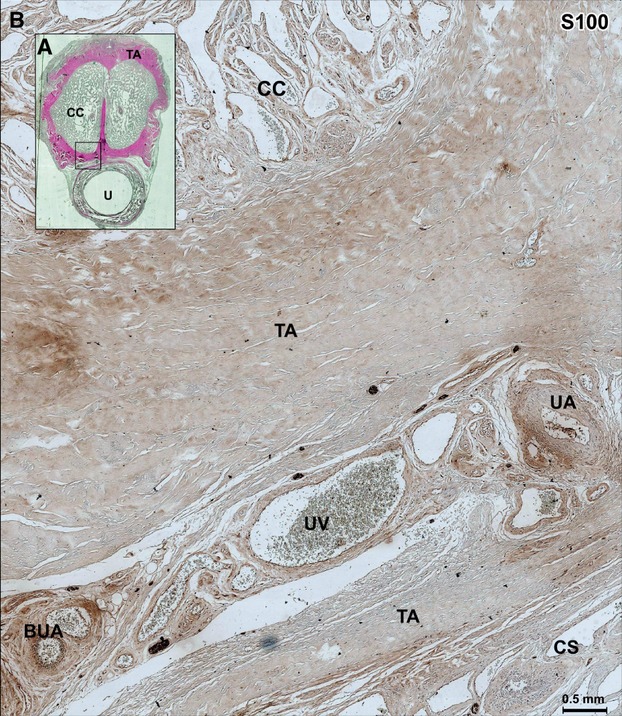
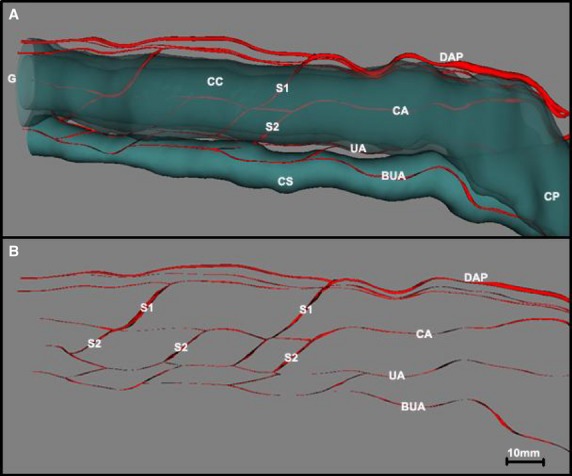
The purpose of this study was to identify the microscopic arterial vascularization of the corpora cavernosa (CC) of the penis using computer-assisted anatomic dissection (CAAD), determine the contribution of the different penile arteries towards this vascularization, detail the nature of cavernospongiosum shunts, and locate the anastomoses between these different arteries. Tissue specimens were taken from five donors who donated their bodies to science. The specimens were fixed in 10% formalin and sliced into a series of five 5-μm sections at intervals of 200 μm. The first section was stained with hematoxylin-eosin or Masson's trichrome and the second with anti-protein S100. The cavernous artery of the penis is not the only source of arterial vascularization of the CC. In four of the five cases studied, we found two to four perforating branches arising from the dorsal arteries of the penis that join up with the cavernous artery of the penis or that are solely responsible for the vascularization of the distal third of the penis. The bulbo-urethral and urethral arteries are situated outside of the tunica albuginea of the corpus spongiosum on their lateral and dorsal sides. The anastomoses do not occur between the cavernous artery of the penis and the corpus spongiosum but between the cavernous artery of the penis and the urethral artery on the surface of the tunica albuginea. All of these arteries are accompanied by nerve branches. The CC were found to be vascularized by both cavernous and dorsal arteries of the penis. Intrapenile vascularization is organized around four arterial axes, which are anastomosed by multiple neurovascular shunts.
Keywords: cavernous artery; cavernous urethral shunt; corpora cavernosa; erection; penis.
© 2013 Anatomical Society.
Figures

References
-
- Bookstein JJ, Lang EV. Penile magnification pharmacoarteriography: details of intrapenile arterial anatomy. Am J Roentgenol. 1987;148:883–888. - PubMed
-
- Conti G. The erection of the human penis and its morphologico-vascular basis. Acta Anat (Basel) 1952;14:217–262. - PubMed
-
- Costabile RA, Spevak M, Fishman IJ, et al. Efficacy and safety of transurethral alprostadil in patients with erectile dysfunction following radical prostatectomy. J Urol. 1998;160:1325–1328. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
