

Chronic kidney disease of uncertain aetiology: prevalence and causative factors in a developing country
- PMID: 23981540
- PMCID: PMC3765913
- DOI: 10.1186/1471-2369-14-180
Chronic kidney disease of uncertain aetiology: prevalence and causative factors in a developing country
Abstract
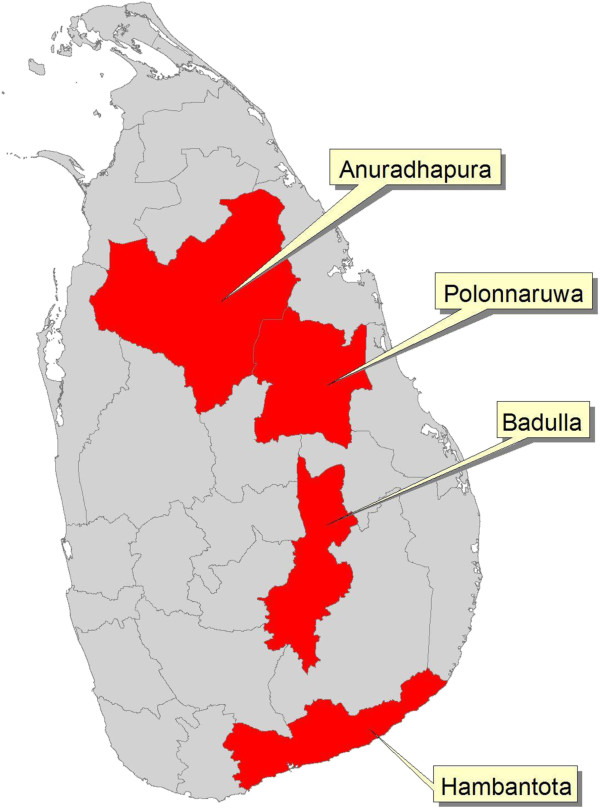
Background: This study describes chronic kidney disease of uncertain aetiology (CKDu), which cannot be attributed to diabetes, hypertension or other known aetiologies, that has emerged in the North Central region of Sri Lanka.
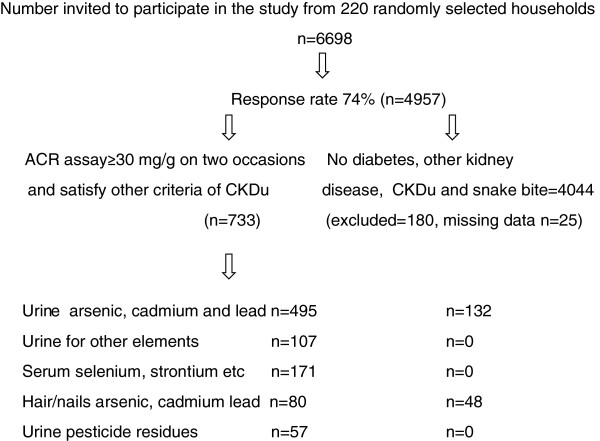
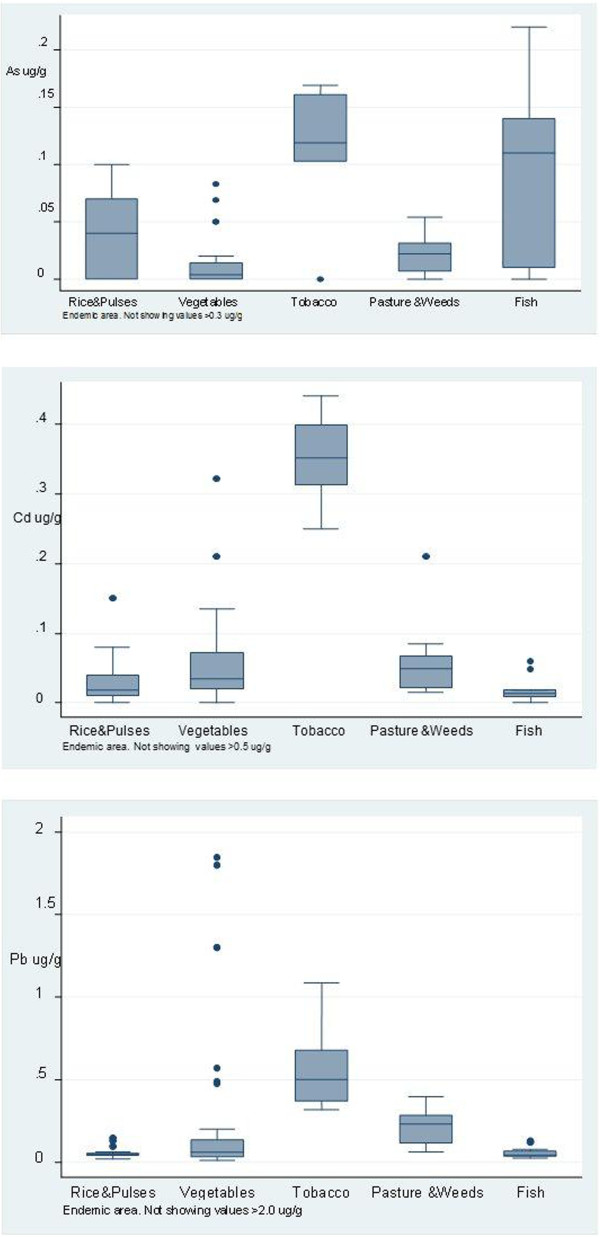
Methods: A cross-sectional study was conducted, to determine the prevalence of and risk factors for CKDu. Arsenic, cadmium, lead, selenium, pesticides and other elements were analysed in biological samples from individuals with CKDu and compared with age- and sex-matched controls in the endemic and non-endemic areas. Food, water, soil and agrochemicals from both areas were analysed for heavy metals.
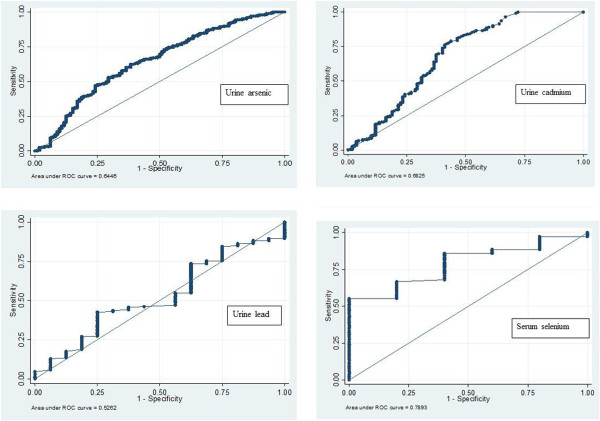
Results: The age-standardised prevalence of CKDu was 12.9% (95% confidence interval [CI] = 11.5% to 14.4%) in males and 16.9% (95% CI = 15.5% to 18.3%) in females. Severe stages of CKDu were more frequent in males (stage 3: males versus females = 23.2% versus 7.4%; stage 4: males versus females = 22.0% versus 7.3%; P < 0.001). The risk was increased in individuals aged >39 years and those who farmed (chena cultivation) (OR [odds ratio] = 1.926, 95% CI = 1.561 to 2.376 and OR = 1.195, 95% CI = 1.007 to 1.418 respectively, P < 0.05). The risk was reduced in individuals who were male or who engaged in paddy cultivation (OR = 0.745, 95% CI = 0.562 to 0.988 and OR = 0.732, 95% CI = 0.542 to 0.988 respectively, P < 0.05). The mean concentration of cadmium in urine was significantly higher in those with CKDu (1.039 μg/g) compared with controls in the endemic and non-endemic areas (0.646 μg/g, P < 0.001 and 0.345 μg/g, P < 0.05) respectively. Urine cadmium sensitivity and specificity were 70% and 68.3% respectively (area under the receiver operating characteristic curve = 0.682, 95% CI = 0.61 to 0.75, cut-off value ≥0.397 μg/g). A significant dose-effect relationship was seen between urine cadmium concentration and CKDu stage (P < 0.05). Urine cadmium and arsenic concentrations in individuals with CKDu were at levels known to cause kidney damage. Food items from the endemic area contained cadmium and lead above reference levels. Serum selenium was <90 μg/l in 63% of those with CKDu and pesticides residues were above reference levels in 31.6% of those with CKDu.
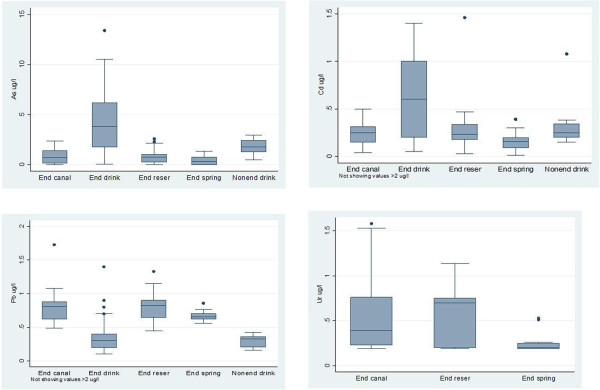
Conclusions: These results indicate chronic exposure of people in the endemic area to low levels of cadmium through the food chain and also to pesticides. Significantly higher urinary excretion of cadmium in individuals with CKDu, and the dose-effect relationship between urine cadmium concentration and CKDu stages suggest that cadmium exposure is a risk factor for the pathogensis of CKDu. Deficiency of selenium and genetic susceptibility seen in individuals with CKDu suggest that they may be predisposing factors for the development of CKDu.
Figures
Comment in
-
Additional perspectives on chronic kidney disease of unknown aetiology (CKDu) in Sri Lanka--lessons learned from the WHO CKDu population prevalence study.BMC Nephrol. 2014 Jul 28;15:125. doi: 10.1186/1471-2369-15-125. BMC Nephrol. 2014. PMID: 25069485 Free PMC article.
-
Response.BMC Nephrol. 2014;15:125. BMC Nephrol. 2014. PMID: 25147882 No abstract available.
References
-
- Nanayakkara S, Komiya T, Ratnatunga N, Senevirathna ST, Harada KH, Hitomi T, Gobe G, Muso E, Abeysekera T, Koizumi A. Tubulointerstitial damage as the major pathological lesion in endemic chronic kidney disease among farmers in North Central Province of Sri Lanka. Environ Health Prev Med. 2012;17:213–221. doi: 10.1007/s12199-011-0243-9. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
