

The role of potentially preventable hospital exposures in the development of acute respiratory distress syndrome: a population-based study
- PMID: 23982022
- PMCID: PMC3844124
- DOI: 10.1097/CCM.0b013e318298a6db
The role of potentially preventable hospital exposures in the development of acute respiratory distress syndrome: a population-based study
Abstract
Objective: Acute respiratory distress syndrome is a common complication of critical illness, with high mortality and limited treatment options. Preliminary studies suggest that potentially preventable hospital exposures contribute to acute respiratory distress syndrome development. We aimed to determine the association between specific hospital exposures and the rate of acute respiratory distress syndrome development among at-risk patients.
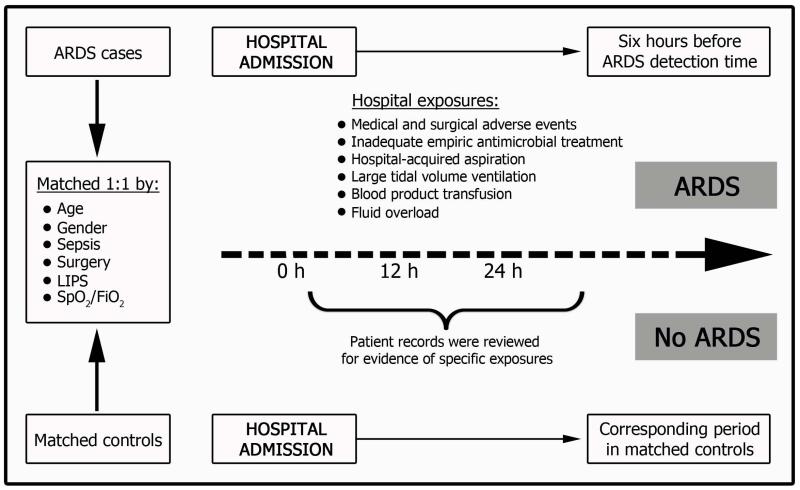
Design: Population-based, nested, Matched case-control study.
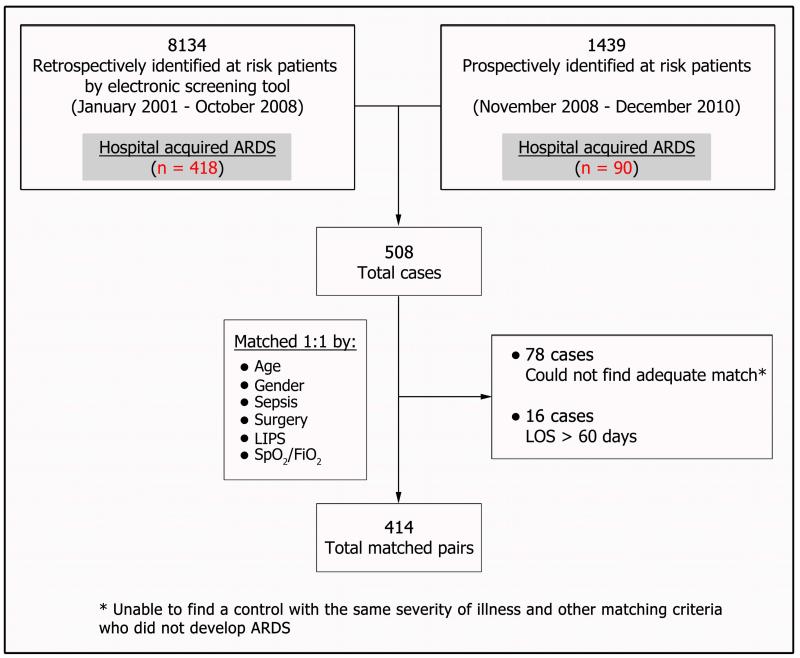
Patients: Consecutive adults who developed acute respiratory distress syndrome from January 2001 through December 2010 during their hospital stay (cases) were matched to similar-risk patients without acute respiratory distress syndrome (controls). They were matched for 6 baseline characteristics.
Interventions: None.
Measurements and main results: Trained investigators blinded to outcome of interest reviewed medical records for evidence of specific exposures, including medical and surgical adverse events, inadequate empirical antimicrobial treatment, hospital-acquired aspiration, injurious mechanical ventilation, transfusion, and fluid and medication administration. Conditional logistic regression was used to calculate the risk associated with individual exposures. During the 10-year period, 414 patients with hospital-acquired acute respiratory distress syndrome were identified and matched to 414 at-risk, acute respiratory distress syndrome-free controls. Adverse events were highly associated with acute respiratory distress syndrome development (odds ratio, 6.2; 95% CI, 4.0-9.7), as were inadequate antimicrobial therapy, mechanical ventilation with injurious tidal volumes, hospital-acquired aspiration, and volume of blood products transfused and fluids administered. Exposure to antiplatelet agents during the at-risk period was associated with a decreased risk of acute respiratory distress syndrome. Rate of adverse hospital exposures and prevalence of acute respiratory distress syndrome decreased during the study period.
Conclusions: Prevention of adverse hospital exposures in at-risk patients may limit the development of acute respiratory distress syndrome.
Figures
Comment in
-
Designing a better "nest": applicable to preventing hospital exposures to risk factors for acute respiratory distress syndrome or just retrospective study design?Crit Care Med. 2014 Jan;42(1):197-8. doi: 10.1097/CCM.0b013e3182a11eab. Crit Care Med. 2014. PMID: 24346523 Free PMC article. No abstract available.
References
-
- Ware LB, Matthay MA. The acute respiratory distress syndrome. N Engl J Med. 2000;342(18):1334–1349. - PubMed
-
- Phua J, Badia JR, Adhikari NK, et al. Has mortality from acute respiratory distress syndrome decreased over time?: A systematic review. American Journal of Respiratory and Critical Care Medicine. 2009;179(3):220–227. - PubMed
-
- Rubenfeld GD, Herridge MS. Epidemiology and Outcomes of Acute Lung Injury 10.1378/chest.06-1976. Chest. 2007;131(2):554–562. - PubMed
-
- Yilmaz M, Keegan MT, Iscimen R, et al. Toward the prevention of acute lung injury: protocol-guided limitation of large tidal volume ventilation and inappropriate transfusion. Crit Care Med. 2007;35(7):1660–1666. quiz 1667. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
