

Causes, risk factors, and trends in failures after TKA in Korea over the past 5 years: a multicenter study
- PMID: 23982406
- PMCID: PMC3889422
- DOI: 10.1007/s11999-013-3252-8
Causes, risk factors, and trends in failures after TKA in Korea over the past 5 years: a multicenter study
Abstract
Background: Failure after total knee arthroplasty (TKA) may be related to emerging technologies, surgical techniques, and changing patient demographics. Over the past decade, TKA use in Korea has increased substantially, and demographic trends have diverged from those of Western countries, but failure mechanisms in Korea have not been well studied.
Questions/purposes: We determined the causes of failure after TKA, the risk factors for failure, and the trends in revision TKAs in Korea over the last 5 years.
Methods: We retrospectively reviewed 634 revision TKAs and 20,234 primary TKAs performed at 19 institutes affiliated with the Kleos Korea Research Group from 2008 to 2012. We recorded the causes of failure after TKA using 11 complications from the standardized complication list of The Knee Society, patient demographics, information on index and revision of TKAs, and indications for index TKA. The influences of patient demographics and indications for index TKA on the risk of TKA failure were evaluated using multivariate regression analysis. The trends in revision procedures and demographic features of the patients undergoing revision TKA over the last 5 years were assessed.
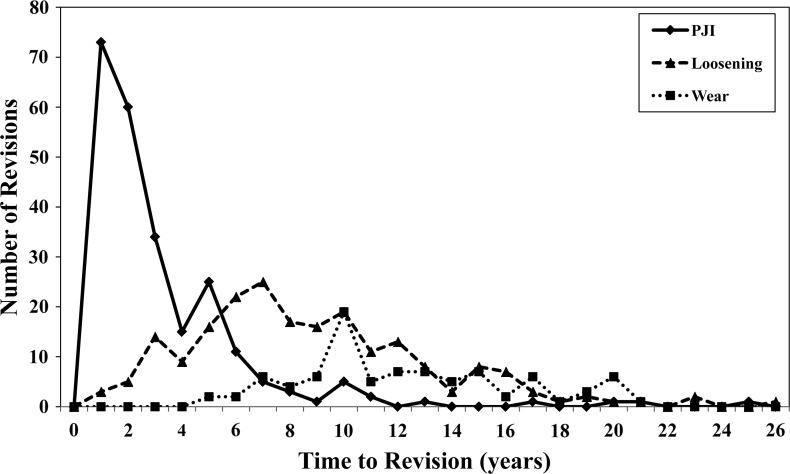
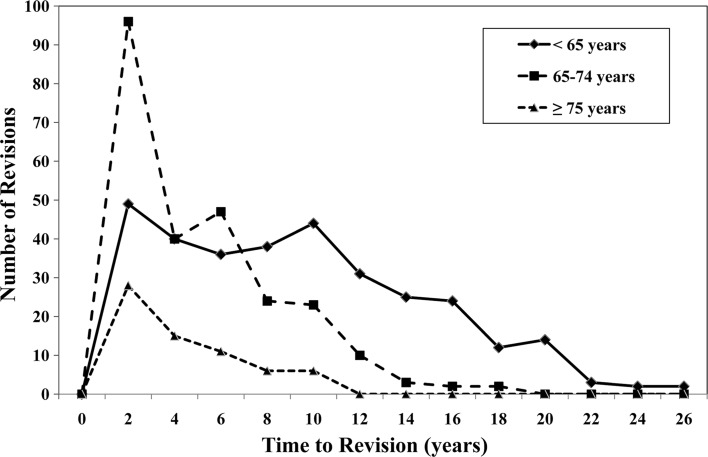
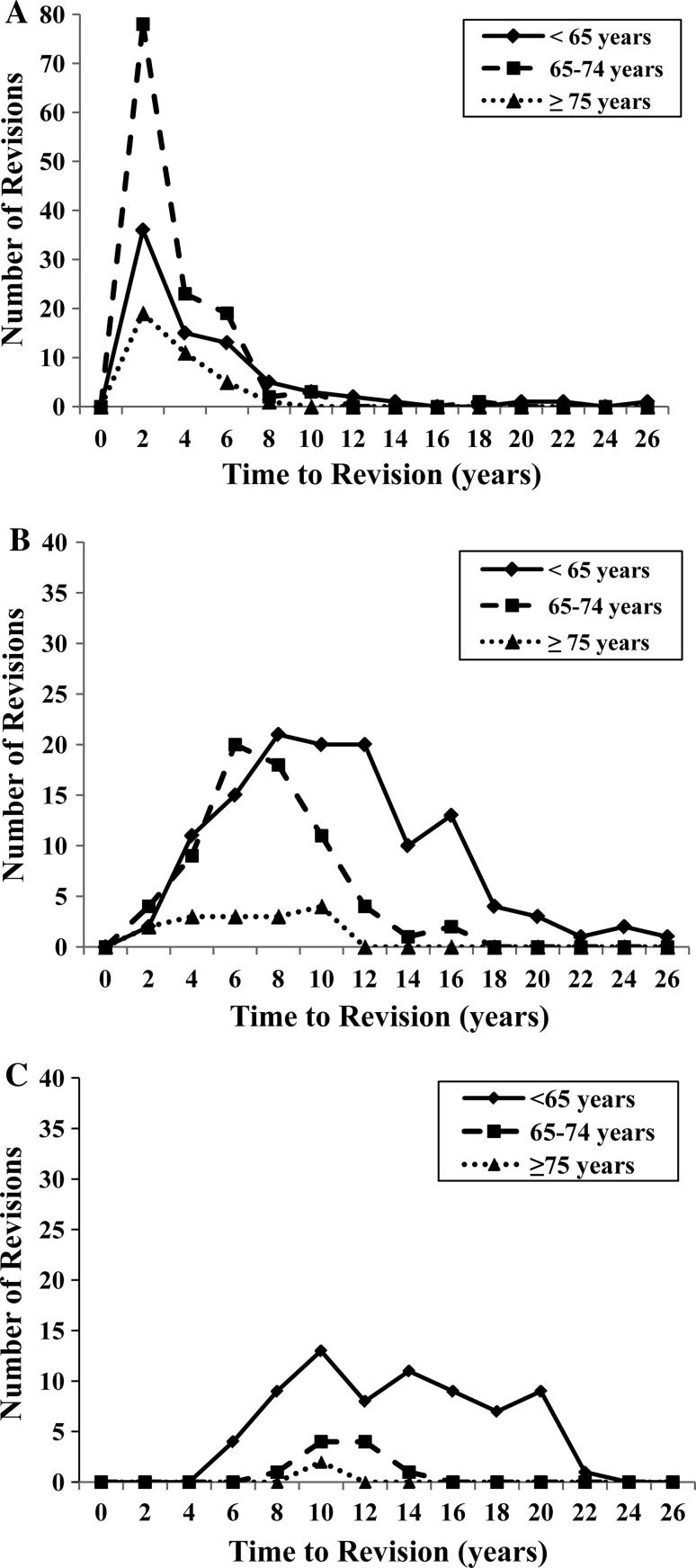
Results: The most common cumulative cause of TKA failure was infection (38%) followed by loosening (33%), wear (13%), instability (7%), and stiffness (3%). However, the incidence of infections has declined over the past 5 years, whereas that of loosening has increased and exceeds that of infection in the more recent 3 years. Young age (odds ratio [OR] per 10 years of age increase, 0.41; 95% confidence interval [CI], 0.37-0.49) and male sex (OR, 1.88; 95% CI, 1.42-2.49) were associated with an increased risk of failure. The percentage of revision TKAs in all primary and revision TKAs remained at approximately 3%, but the annual numbers of revision TKAs in the more recent 3 years increased from that of 2008 by more than 23%.
Conclusions: Despite a recent remarkable increase in TKA use and differences in demographic features, the causes and risk factors for failures in Korea were similar to those of Western countries. Infection was the most common cause of failure, but loosening has emerged as the most common cause in more recent years, which would prompt us to scrutinize the cause and solution to reduce it.
Figures
Comment in
-
CORR Insights ®: Causes, risk factors, and trends in failures after TKA in Korea over the past 5 years: a multicenter study.Clin Orthop Relat Res. 2014 Jan;472(1):327-8. doi: 10.1007/s11999-013-3286-y. Epub 2013 Sep 24. Clin Orthop Relat Res. 2014. PMID: 24061846 Free PMC article. No abstract available.
References
-
- Australian Orthopaedic Association (AOA). National Joint Replacement Registry (NJRR) Hip and Knee Arthroplasty Annual Report. 2012. Available at: www.dmac.adelaide.edu.au/aoanjrr/documents/AnnualReports2012/AnnualRepor.... Accessed February 10, 2013.
-
- Canadian Institute of Health Information (CIHI). Canadian Joint Replacement Registry (CJRR) Hip and Knee Replacement in Canada 2007 Annual Report. Available at: http://secure.cihi.ca/cihiweb/products/2007CJRRAnnualReport%20(web).pdf. 20. Accessed Feburary 10, 2013.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
