

Update in intracerebral hemorrhage
- PMID: 23983850
- PMCID: PMC3726132
- DOI: 10.1177/1941875211409050
Update in intracerebral hemorrhage
Abstract
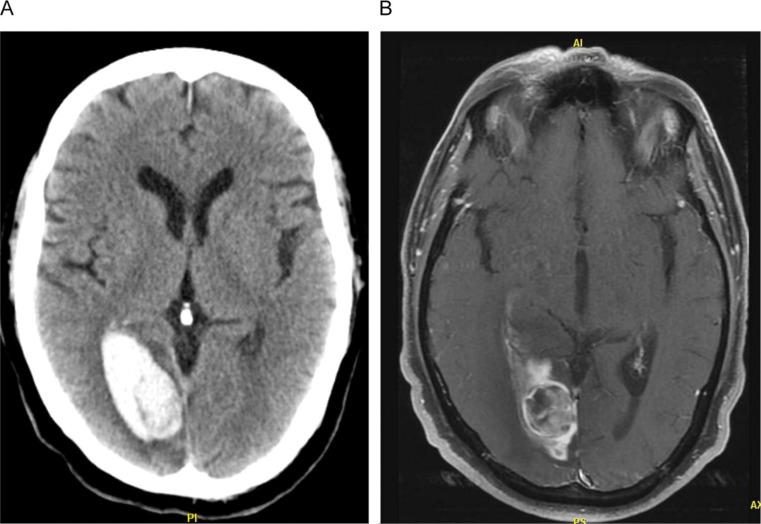
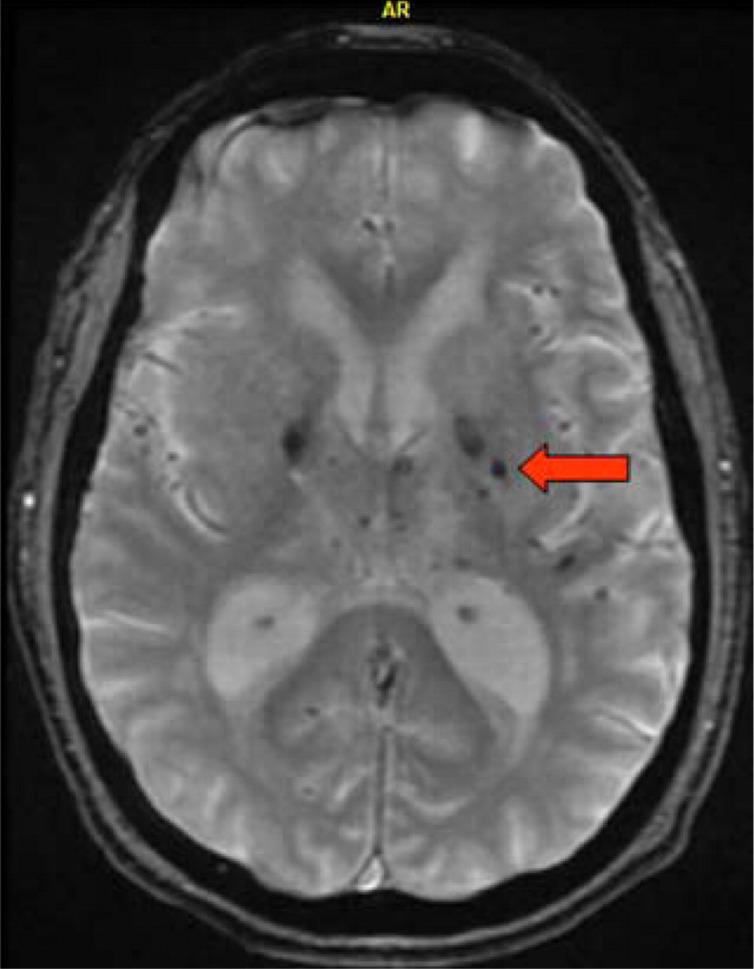
Spontaneous, nontraumatic intracerebral hemorrhage (ICH) is defined as bleeding within the brain parenchyma. Intracranial hemorrhage includes bleeding within the cranial vault and encompasses ICH, subdural hematoma, epidural bleeds, and subarachnoid hemorrhage (SAH). This review will focus only on ICH. This stroke subtype accounts for about 10% of all strokes. The hematoma locations are deep or ganglionic, lobar, cerebellar, and brain stem in descending order of frequency. Intracerebral hemorrhage occurs twice as common as SAH and is equally as deadly. Risk factors for ICH include hypertension, cerebral amyloid angiopathy, advanced age, antithrombotic therapy and history of cerebrovascular disease. The clinical presentation is "stroke like" with sudden onset of focal neurological deficits. Noncontrast head computerized tomography (CT) scan is the standard diagnostic tool. However, newer neuroimaging techniques have improved the diagnostic yield in terms of underlying pathophysiology and may aid in prognosis. Intracerebral hemorrhage is a neurological emergency. Medical care begins with stabilization of airway, breathing function, and circulation (ABCs), followed by specific measures aimed to decrease secondary neurological damage and to prevent both medical and neurological complications. Reversal of coagulopathy when present is of the essence. Blood pressure management can be key and continues as an area of debate and ongoing research. Surgical evacuation of ICH is of unproven benefit though a subset of well-selected patients may have improved outcomes. Ventriculostomy and intracranial pressure (ICP) monitoring are interventions also used in this patient population. To date, hemostatic medications and neuroprotectants have failed to result in clinical improvement. A multidisciplinary approach is recommended, with participation of vascular neurology, vascular neurosurgery, critical care, and rehabilitation medicine as the main players.
Keywords: diagnosis; intracerebral hemorrhage; prognosis; surgery; treatment.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures



References
-
- Flaherty ML, Woo D, Haverbusch M, et al. Racial variations in location and risk of intracerebral hemorrhage. Stroke. 2005;36(5):934–937 - PubMed
-
- Grysiewicz RA, Thomas K, Pandey DK. Epidemiology of ischemic and hemorrhagic stroke: incidence, prevalence, mortality, and risk factors. Neurol Clin. 2008;26(4):871–895 - PubMed
-
- Broderick JP, Adams HP, Jr, Barsan W, et al. Guidelines for the management of spontaneous intracerebral hemorrhage: a statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Stroke. 1999;30(4):905–915 - PubMed
-
- Gebel JM, Broderick JP. Intracerebral hemorrhage. Neurol Clin. 2000;18(2):419–438 - PubMed
-
- Qureshi AI, Tuhrim S, Broderick JP, Batjer HH, Hondo H, Hanley DF. Spontaneous intracerebral hemorrhage. [see comment]. N Engl J Med. 2001;344(19):1450–1460 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources