

Paraneoplastic and other autoimmune disorders of the central nervous system
- PMID: 23983888
- PMCID: PMC3726118
- DOI: 10.1177/1941874412453339
Paraneoplastic and other autoimmune disorders of the central nervous system
Abstract
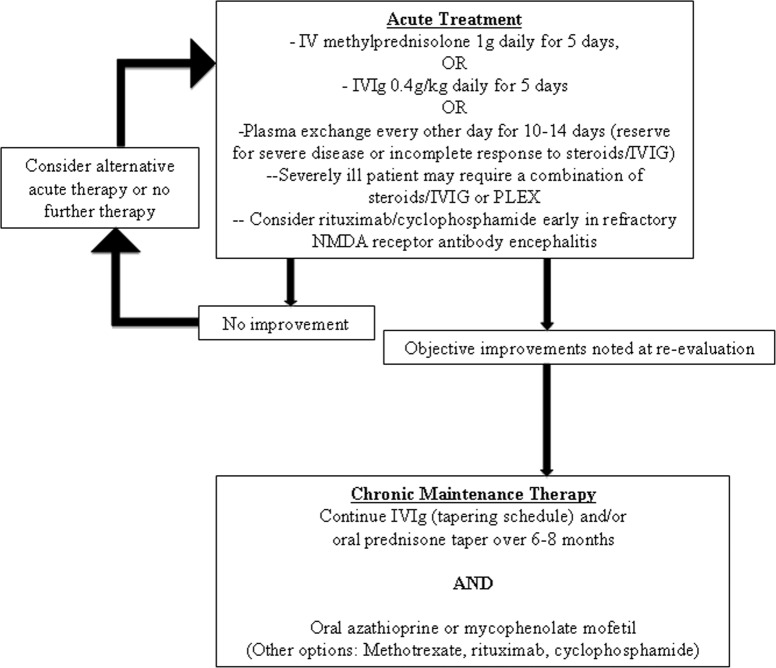
As a result of the burgeoning growth of disease-specific neural autoantibody markers available for diagnostic patient evaluation, there has been increasing awareness of autoimmune central nervous system (CNS) disorders in hospital practice. Hospital-based neurologists have also taken great interest in these disorders since many occur in the setting of an occult systemic cancer which can be detected and treated at an early stage, and many affected patients are responsive to immunotherapy. Associated neurological disorders are typically subacute in onset, some are common or classic (eg, limbic encephalitis, cerebellar degeneration), but others have atypical or multifocal presentations. For patients with a suspected paraneoplastic disorder, many and costly oncological evaluations may be required for diagnosis. Comprehensive serological and cerebrospinal fluid (CSF) evaluation for neural autoantibodies may permit a focused cancer evaluation (eg, antineuronal nuclear antibody type 1 [ANNA-1] is associated with small cell lung carcinoma), and in some circumstances may indicate the likelihood of a good response to therapy (eg, voltage-gated potassium channel complex antibody) or poor neurological prognosis (eg, purkinje cell cytoplasmic antibody type 1 [antiYo]). Positron-emission tomography-computed tomography (PET-CT) imaging of trunk may increase the diagnostic yield for certain cancers where other modalities have been negative. For some patients, rapid treatment with immunotherapy may facilitate marked improvement, or full recovery; multiple sequential trials of one or more of steroids, intravenous immunoglobulin or plasma exchange, or combination therapy are often required. For patients with N-methyl-d-aspartate receptor antibody encephalitis, early treatment with immunosuppressants and weeks or months of supportive intensive care may additionally be required. One or more of clinical examination, electroencephalogram (including video telemetry), and imaging provide objective parameters to which posttreatment outcomes can be compared.
Keywords: Stiff-Person syndrome; myelitis; neuromyelitis optica; transverse.
Conflict of interest statement
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials