

The influence of hemocoagulation disorders on the development of posttraumatic cerebral infarction and outcome in patients with moderate or severe head trauma
- PMID: 23984395
- PMCID: PMC3747364
- DOI: 10.1155/2013/685174
The influence of hemocoagulation disorders on the development of posttraumatic cerebral infarction and outcome in patients with moderate or severe head trauma
Abstract
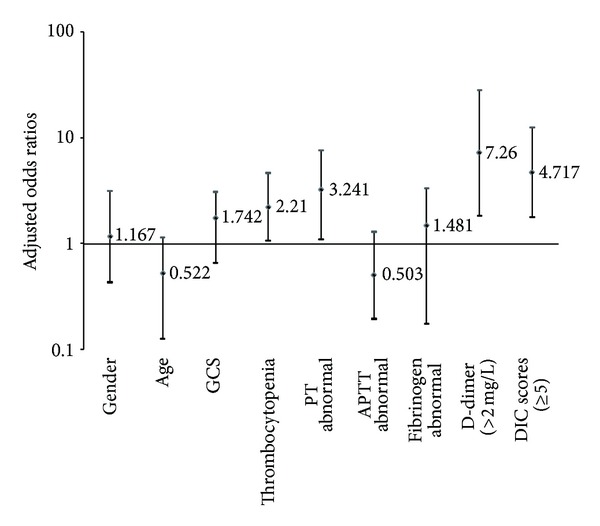
Posttraumatic cerebral infarction (PTCI) is a severe secondary insult of head injury and often leads to a poor prognosis. Hemocoagulation disorder is recognized to have important effects on hemorrhagic or ischemic damages. We sought to assess if posttraumatic hemocoagulation disorders were associated with cerebral infarction, and evaluate their influence on outcome among patients with moderate or severe head trauma. In this study, PTCI was observed in 28 (10.57%) of the 265 patients within the first week after injury. In multivariate analysis, the thrombocytopenia (odds ratio (OR) 2.210, 95% confidence interval (CI) 1.065-4.674), abnormal prothrombin time (PT) (OR 3.241, 95% CI 1.090-7.648), D-dimer (>2 mg/L) (OR 7.260, 95% CI 1.822-28.076), or disseminated intravascular coagulation (DIC) scores (≥ 5) (OR 4.717, 95% CI 1.778-12.517) were each independently associated with an increased risk of PTCI. Admission Glasgow Coma Scale (GCS) score, abnormal activated partial thromboplastin time (APTT) and fibrinogen, and D-dimer (>2 mg/L) and DIC scores (≥ 5) showed an independent predictive effect on poor outcome. In conclusion, recognition of this important treatable cause of PTCI and the associated risk factors may help identify the group at risk and tailor management of patients with TBI.
Figures


References
-
- Alexiou GA, Pahatouridis D, Voulgaris S. Coagulopathy in traumatic brain injury. Injury. 2011;42(1):113–114. - PubMed
-
- Halpern CH, Reilly PM, Turtz AR, Stein SC. Traumatic coagulopathy: the effect of brain injury. Journal of Neurotrauma. 2008;25(8):997–1001. - PubMed
-
- Marino R, Gasparotti R, Pinelli L, et al. Posttraumatic cerebral infarction in patients with moderate or severe head trauma. Neurology. 2006;67(7):1165–1171. - PubMed
-
- Tawil I, Stein DM, Mirvis SE, Scalea TM. Posttraumatic cerebral infarction: incidence, outcome, and risk factors. Journal of Trauma. 2008;64(4):849–853. - PubMed
-
- Tian H-L, Geng Z, Cui Y-H, et al. Risk factors for posttraumatic cerebral infarction in patients with moderate or severe head trauma. Neurosurgical Review. 2008;31(4):431–436. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
