

Detection of cytomegalovirus drug resistance mutations by next-generation sequencing
- PMID: 23985916
- PMCID: PMC3889754
- DOI: 10.1128/JCM.01605-13
Detection of cytomegalovirus drug resistance mutations by next-generation sequencing
Abstract
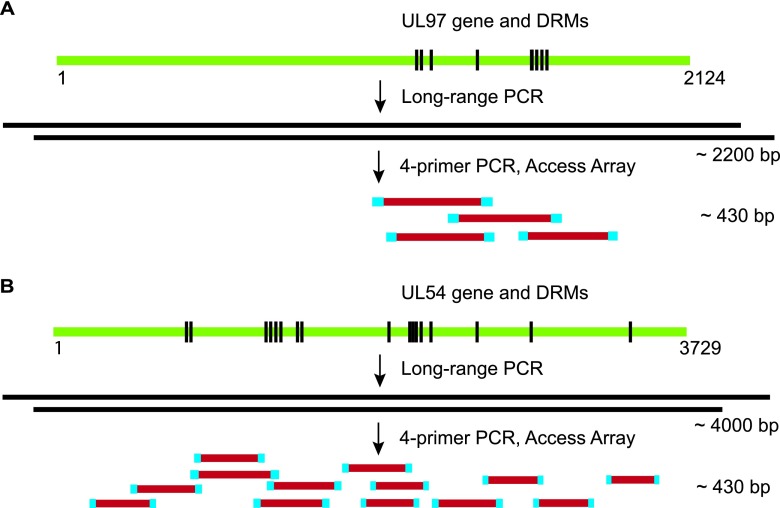
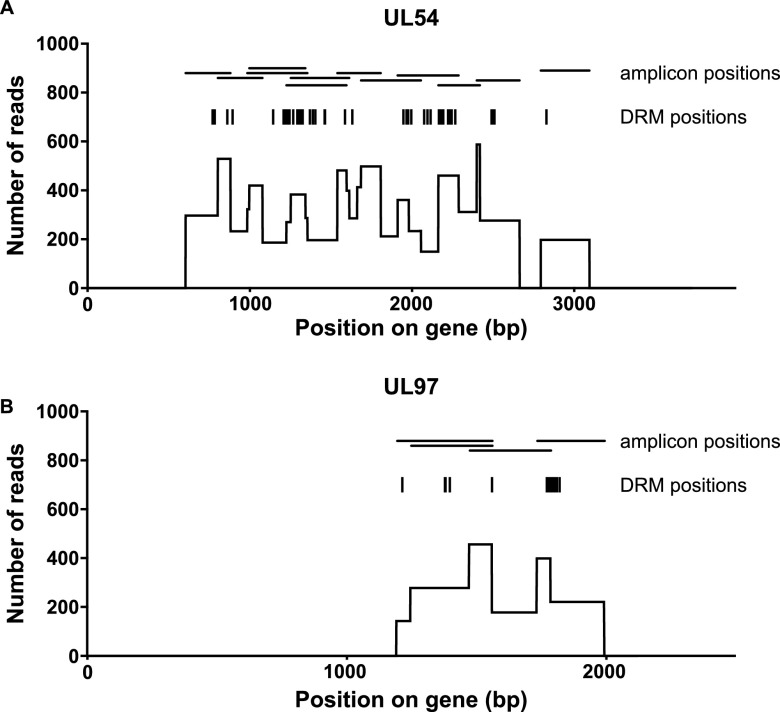
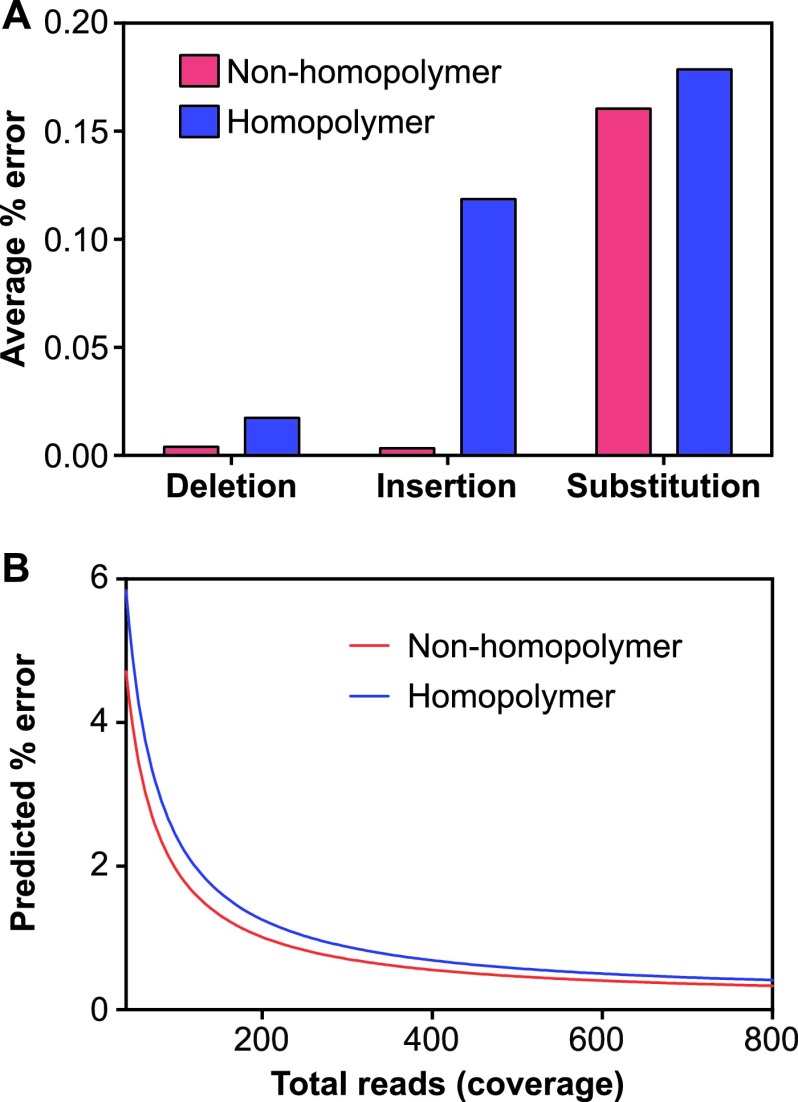
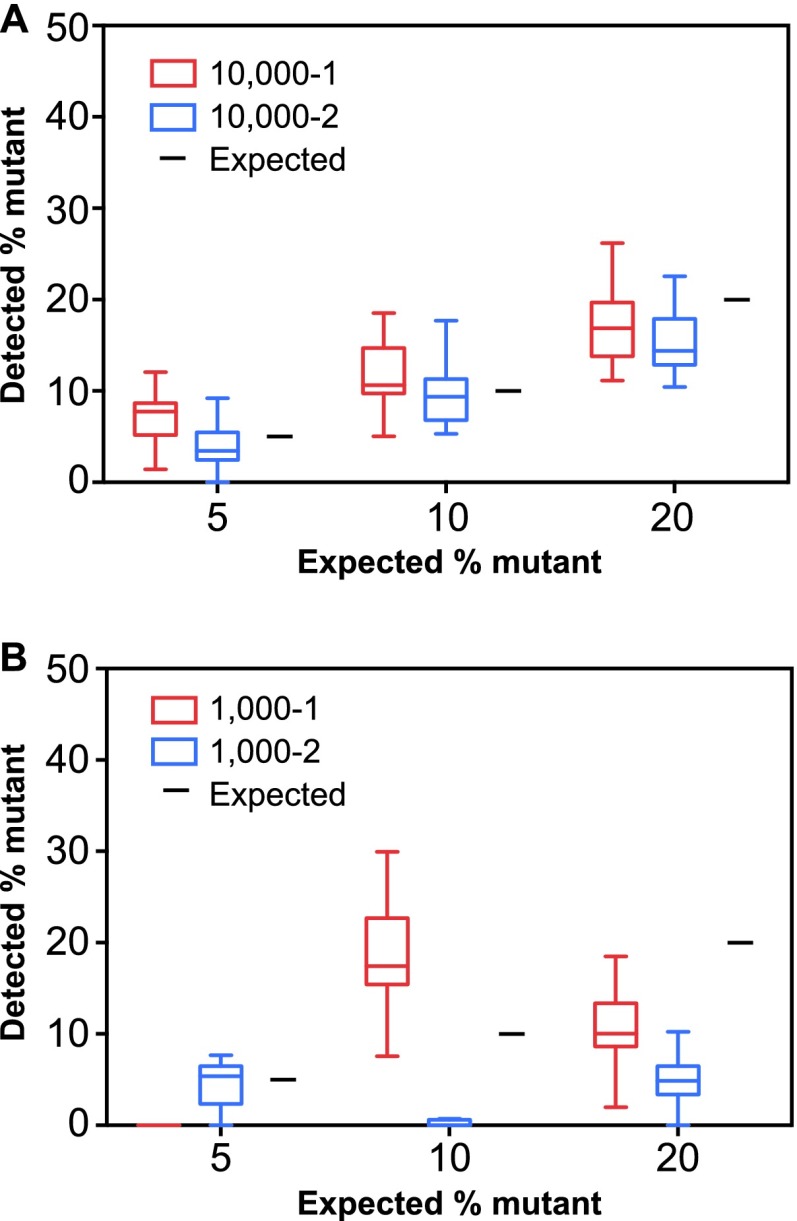
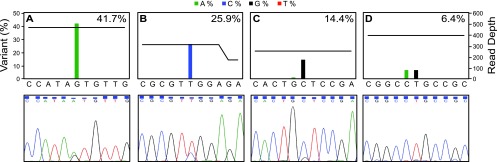
Antiviral therapy for cytomegalovirus (CMV) plays an important role in the clinical management of solid organ and hematopoietic stem cell transplant recipients. However, CMV antiviral therapy can be complicated by drug resistance associated with mutations in the phosphotransferase UL97 and the DNA polymerase UL54. We have developed an amplicon-based high-throughput sequencing strategy for detecting CMV drug resistance mutations in clinical plasma specimens using a microfluidics PCR platform for multiplexed library preparation and a benchtop next-generation sequencing instrument. Plasmid clones of the UL97 and UL54 genes were used to demonstrate the low overall empirical error rate of the assay (0.189%) and to develop a statistical algorithm for identifying authentic low-abundance variants. The ability of the assay to detect resistance mutations was tested with mixes of wild-type and mutant plasmids, as well as clinical CMV isolates and plasma samples that were known to contain mutations that confer resistance. Finally, 48 clinical plasma specimens with a range of viral loads (394 to 2,191,011 copies/ml plasma) were sequenced using multiplexing of up to 24 specimens per run. This led to the identification of seven resistance mutations, three of which were present in <20% of the sequenced population. Thus, this assay offers more sensitive detection of minor variants and a higher multiplexing capacity than current methods for the genotypic detection of CMV drug resistance mutations.
Figures
References
-
- Baroco AL, Oldfield EC. 2008. Gastrointestinal cytomegalovirus disease in the immunocompromised patient. Curr. Gastroenterol. Rep. 10:409–416 - PubMed
-
- Castagnola E, Cappelli B, Erba D, Rabagliati A, Lanino E, Dini G. 2004. Cytomegalovirus infection after bone marrow transplantation in children. Hum. Immunol. 65:416–422 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
