

Tuberculosis of the genitourinary system-Urinary tract tuberculosis: Renal tuberculosis-Part I
- PMID: 23986618
- PMCID: PMC3737618
- DOI: 10.4103/0971-3026.113615
Tuberculosis of the genitourinary system-Urinary tract tuberculosis: Renal tuberculosis-Part I
Abstract
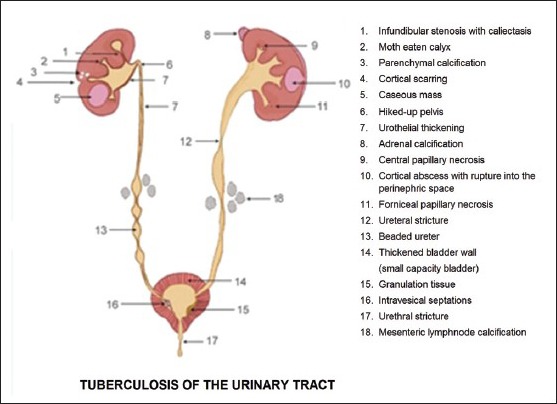
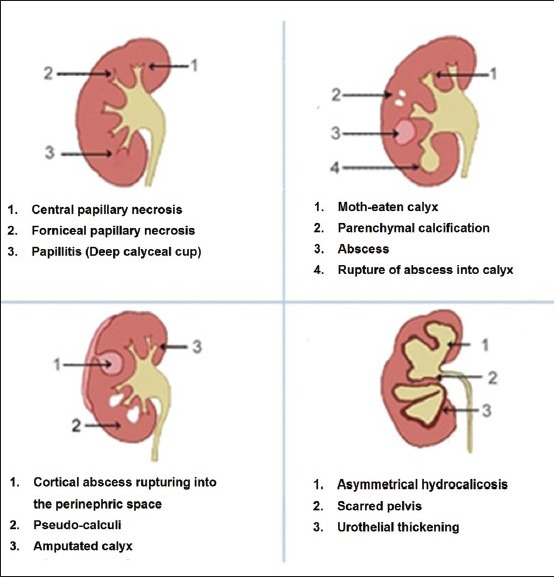
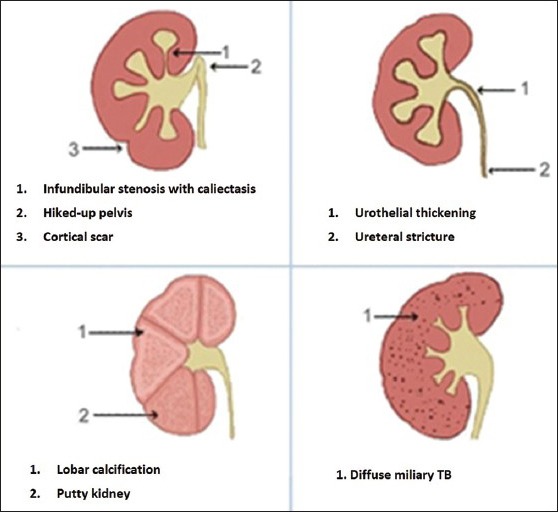
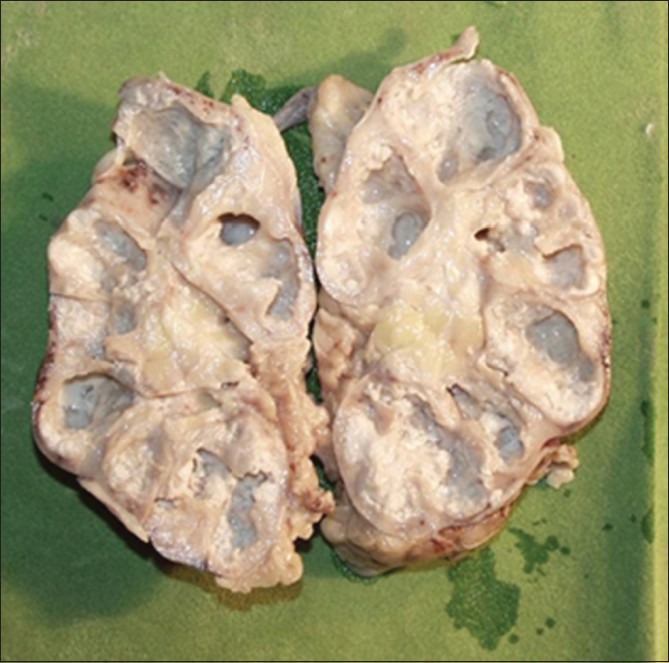
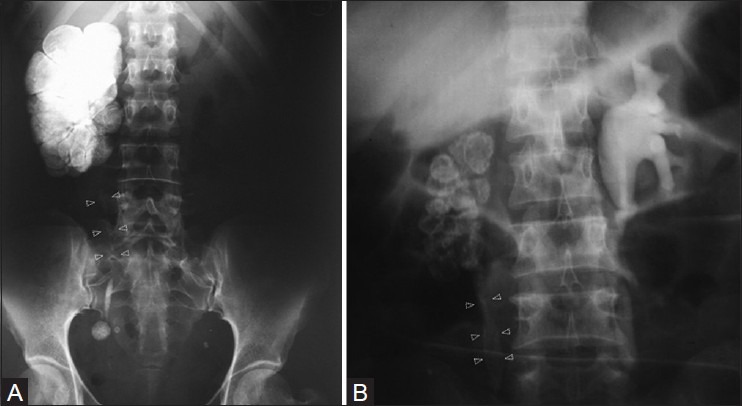
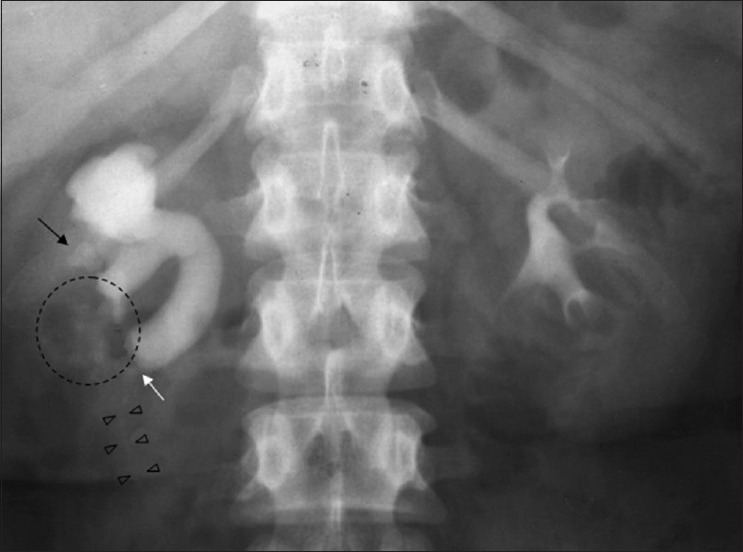
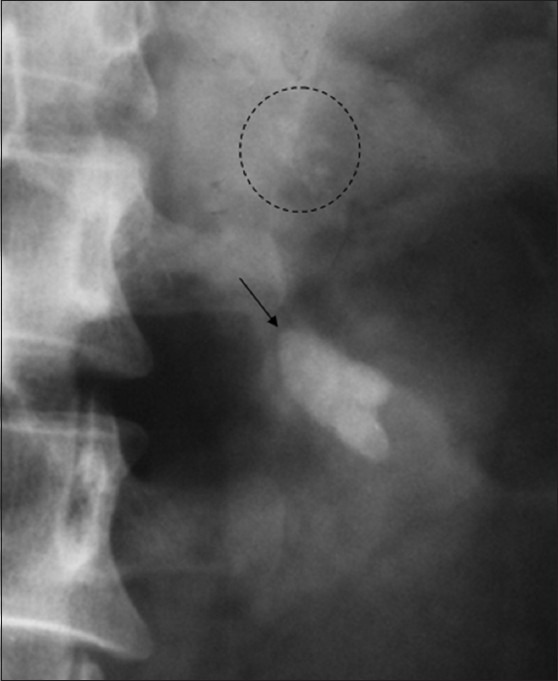
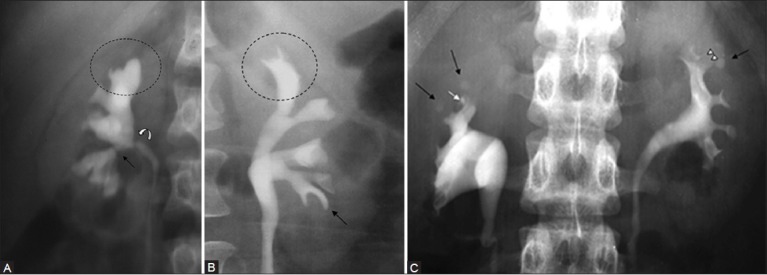
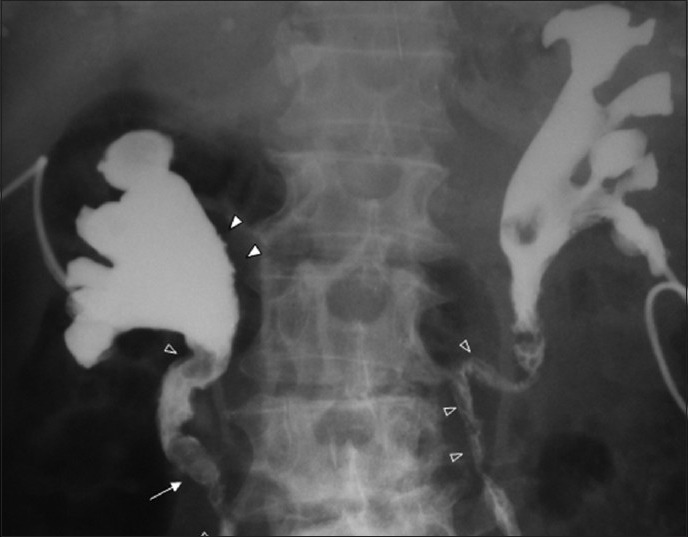
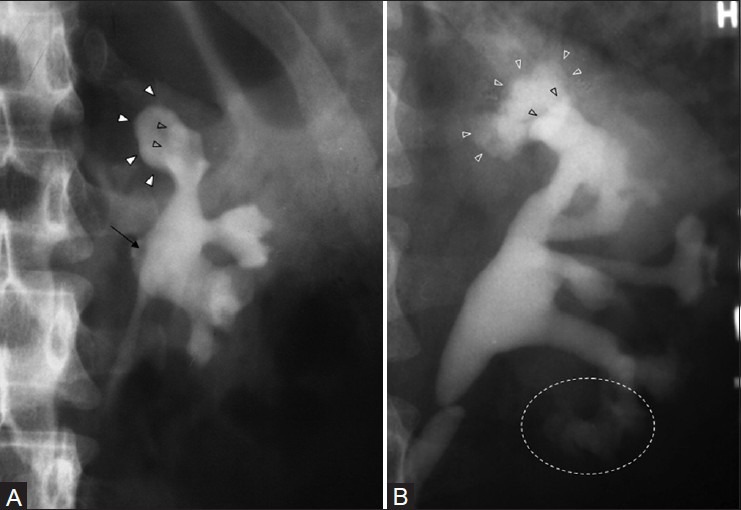
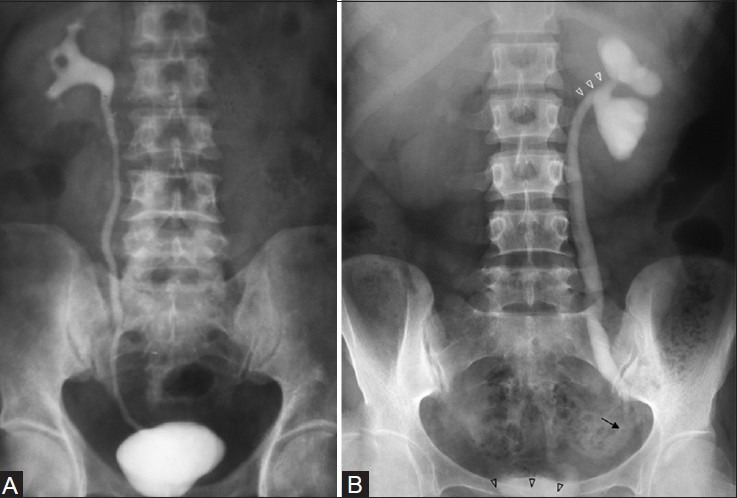
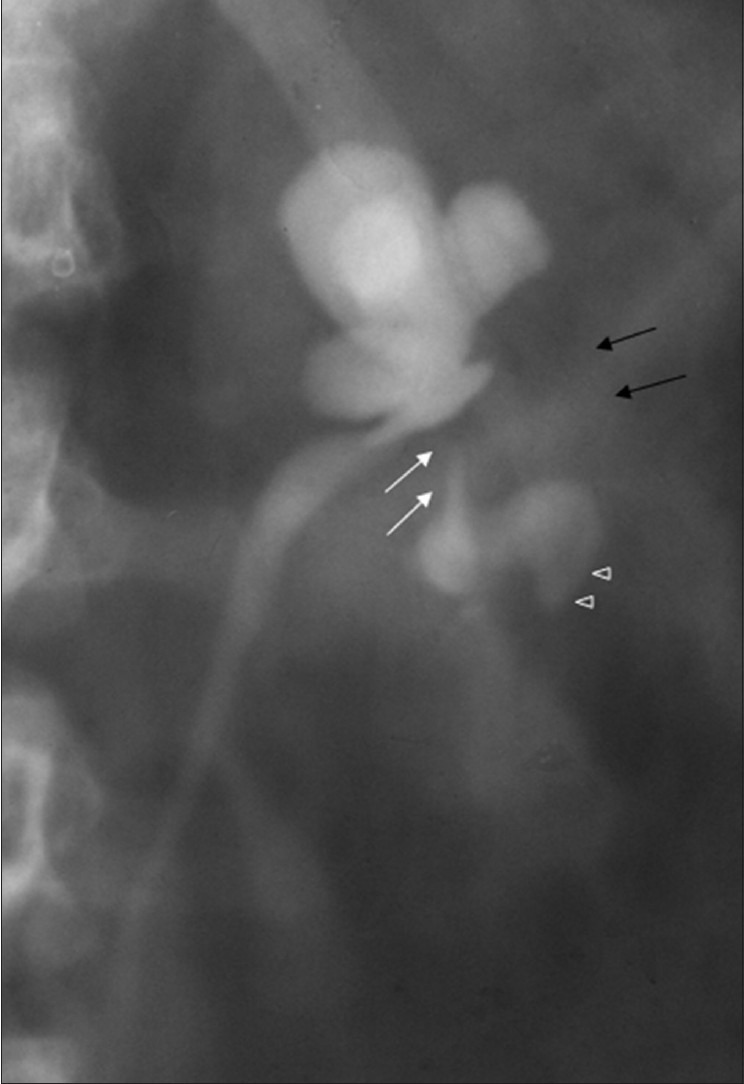
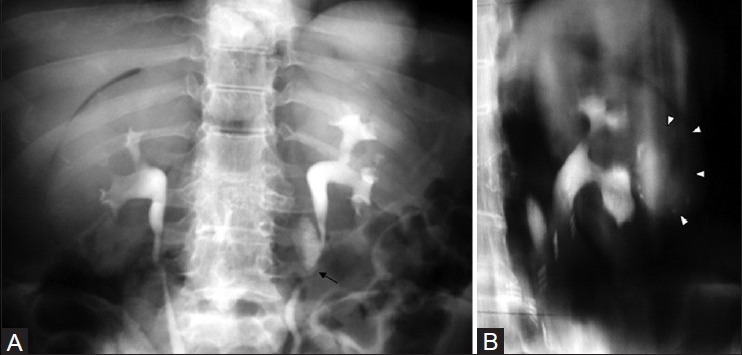
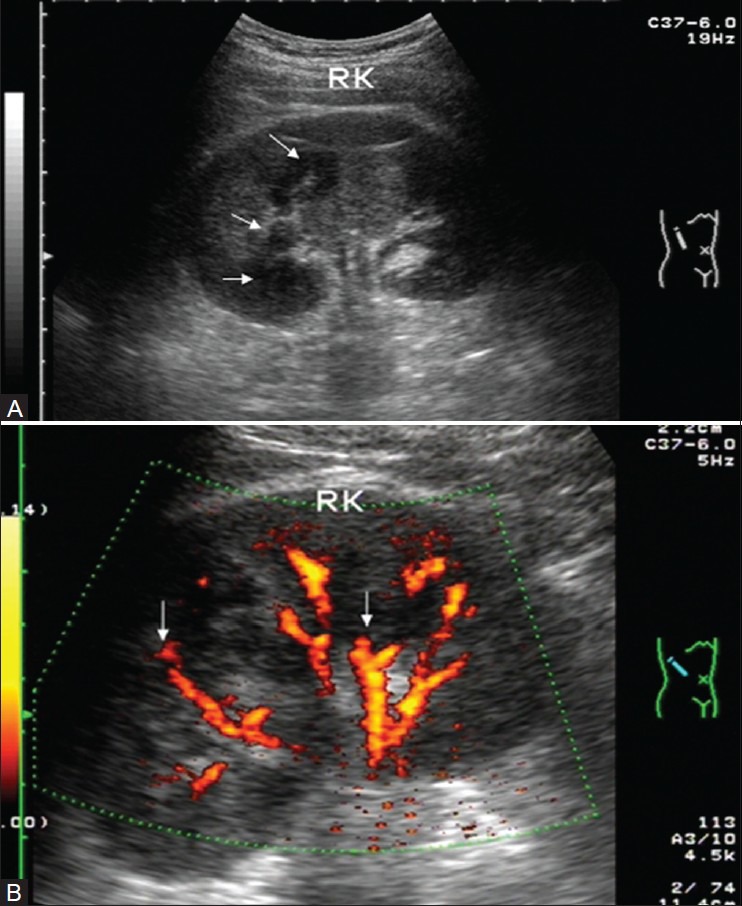
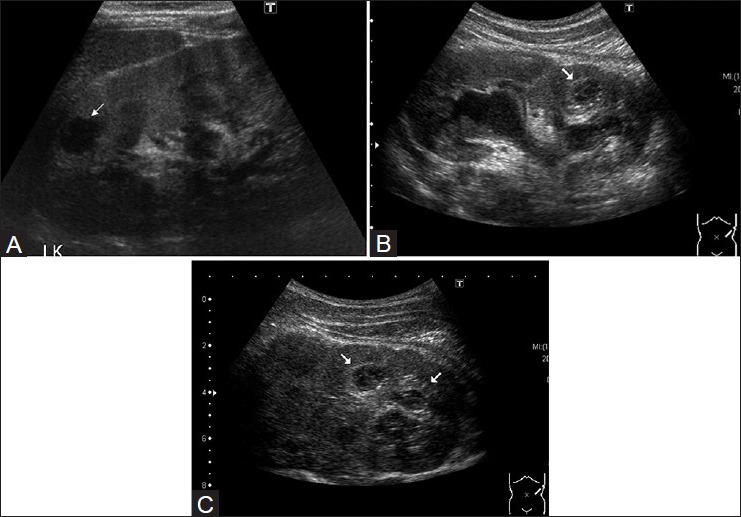
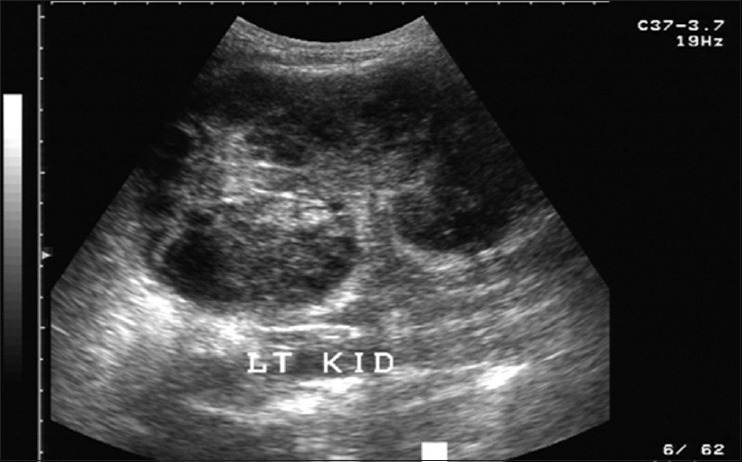
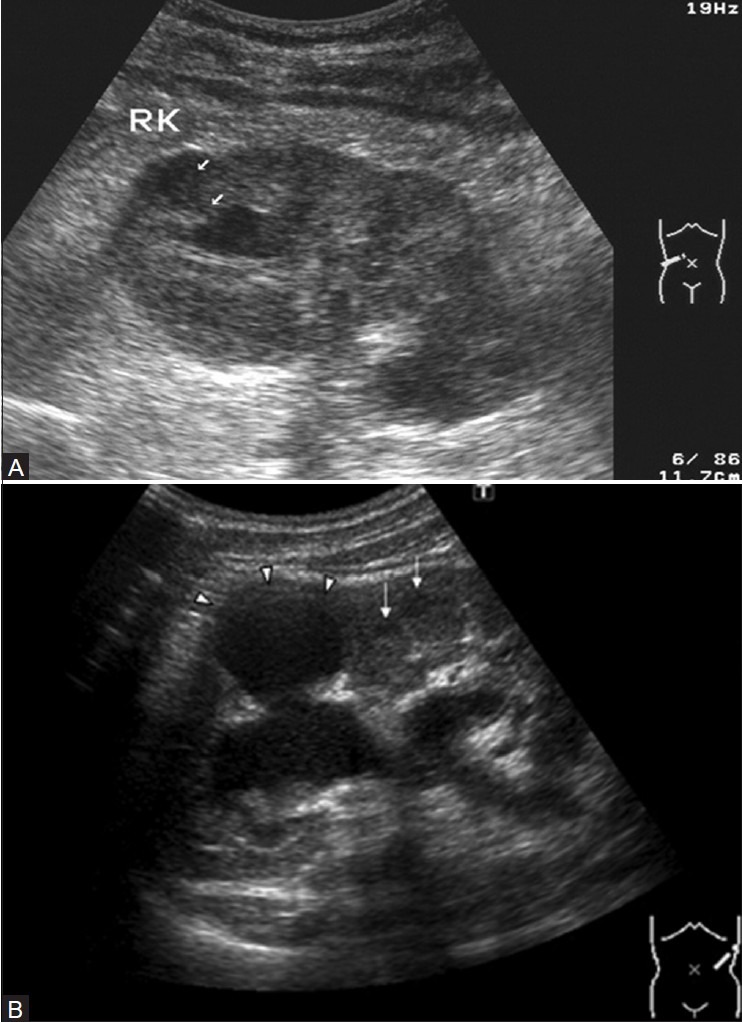
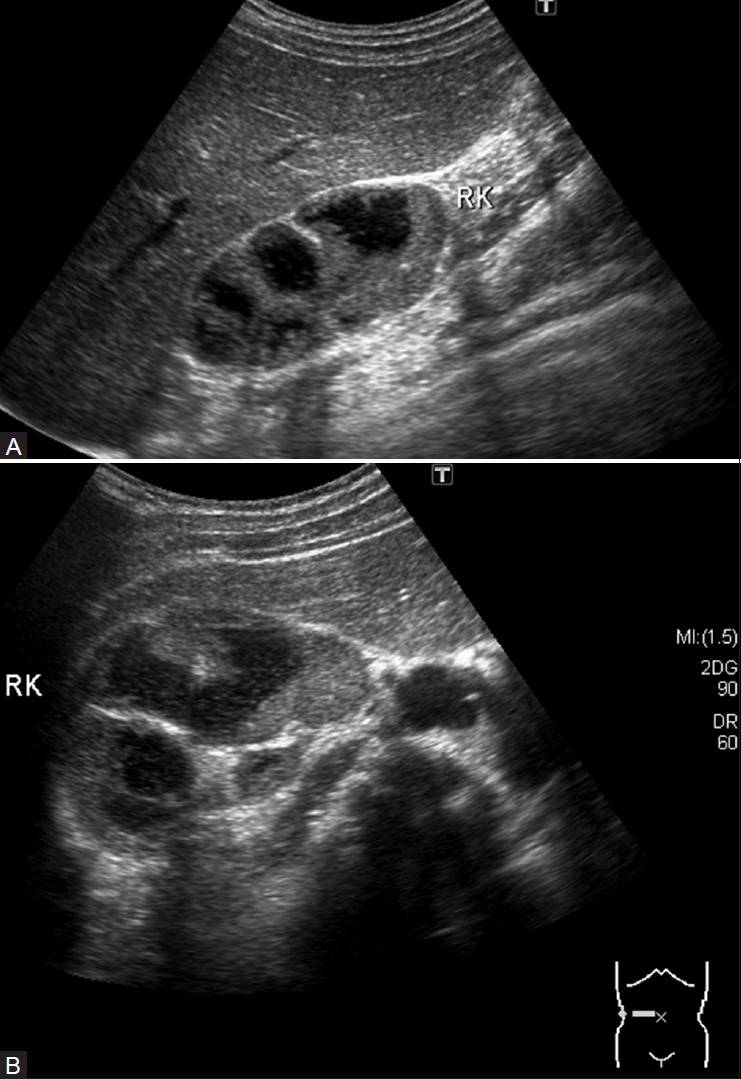
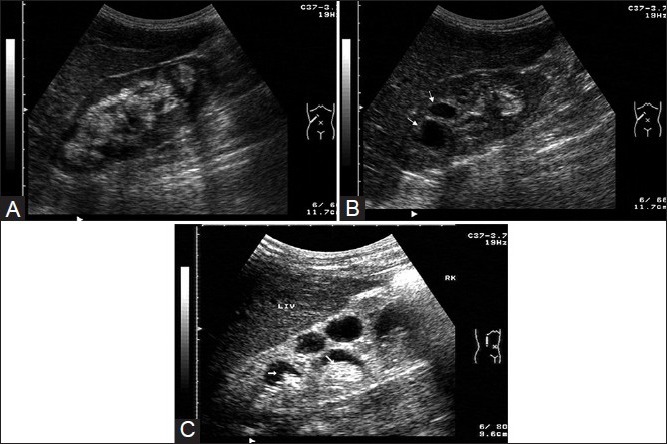
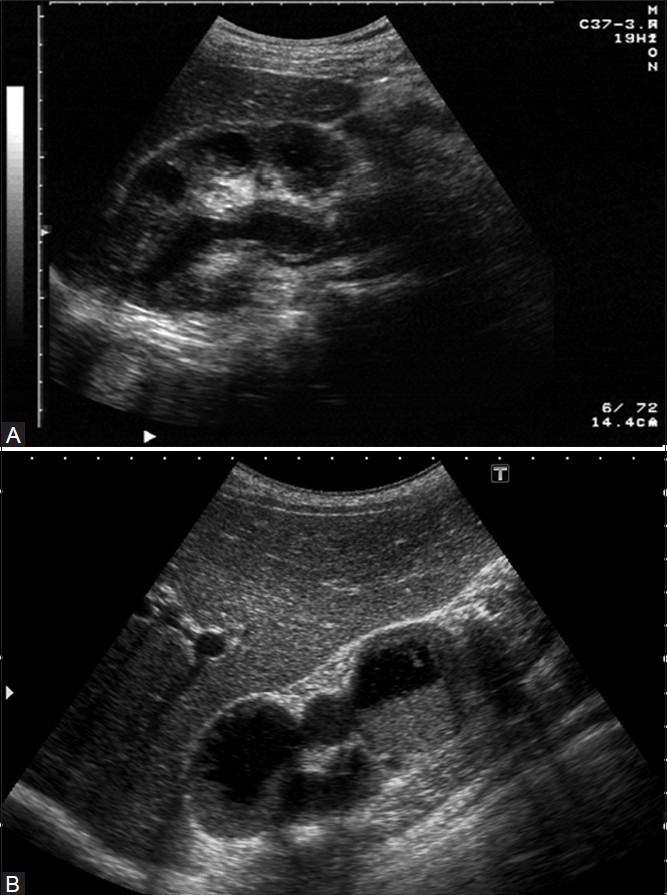
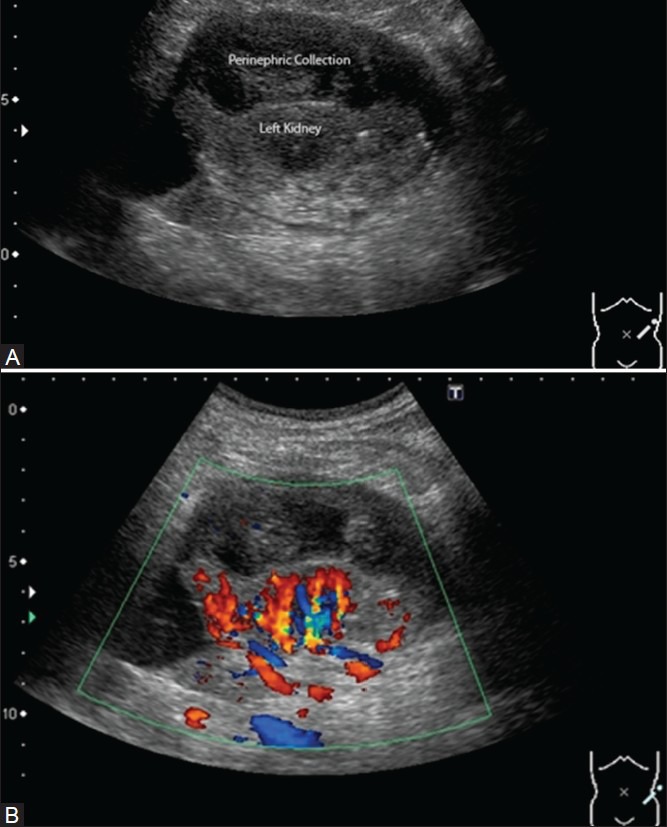
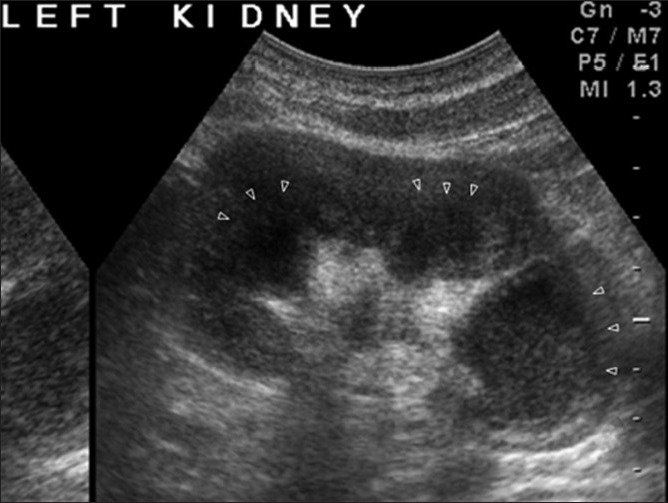
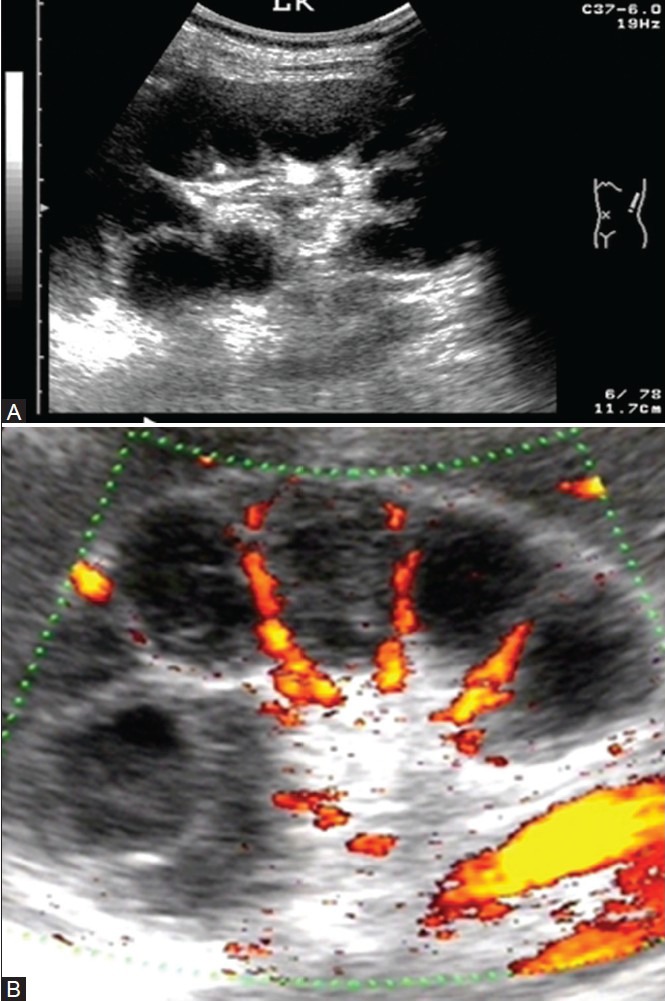
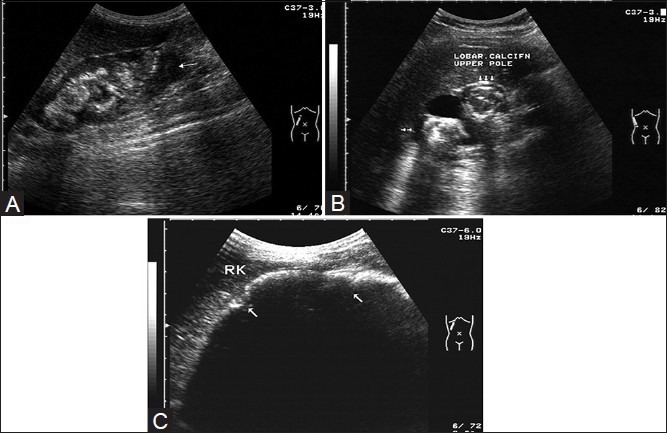
Tuberculosis (TB) remains a worldwide scourge and its incidence appears to be increasing due to various factors, such as the spread of human immunodeficiency virus (HIV) and acquired immunodeficiency syndrome (AIDS). The insidious onset and non-specific constitutional symptoms of genitourinary tuberculosis (GUTB) often lead to delayed diagnosis and rapid progression to a non-functioning kidney. Due to hematogenous dissemination of TB, there is a potential risk of involvement of the contralateral kidney too. Imaging plays an important role in the making of a timely diagnosis and in the planning of treatment, and thus helps to avoid complications such as renal failure. Imaging of GUTB still remains a challenge, mainly on account of the dearth of literature, especially related to the use of the newer modalities such as magnetic resonance imaging (MRI). This two-part article is a comprehensive review of the epidemiology, pathophysiology, and imaging findings in renal TB. Various imaging features of GUTB are outlined, from the pathognomonic lobar calcification on plain film, to finer early changes such as loss of calyceal sharpness and papillary necrosis on intravenous urography (IVU); to uneven caliectasis and urothelial thickening, in the absence of renal pelvic dilatation, as well as the hitherto unreported 'lobar caseation' on ultrasonography (USG). Well-known complications of GUTB such as sinus tracts, fistulae and amyloidosis are described, along with the relatively less well-known complications such as tuberculous interstitial nephritis (TIN), which may remain hidden because of its 'culture negative' nature and thus lead to renal failure. The second part of the article reviews the computed tomography (CT) and MRI features of GUTB and touches upon future imaging techniques along with imaging of TB in transplant recipients and in immunocompromised patients.
Keywords: Renal tuberculosis; intravenous urography; lobar caseation; tuberculous interstitial nephritis; ultrasonography; uneven caliectasis.
Conflict of interest statement
Figures






References
-
- Muttarak M, Chiang Mai WN, Lojanapiwat B. Tuberculosis of the genitourinary tract: Imaging features with pathological correlation. Singapore Med J. 2005;46:568–74. - PubMed
-
- Global tuberculosis control: Key findings from the December 2009 WHO report. Wkly Epidemiol Rec. 2010;85:69–80. - PubMed
-
- Chauhan LS, Tonsing J. Revised national TB control programme in India. Tuberculosis (Edinb) 2005;85:271–6. - PubMed
-
- Burrill J, Williams CJ, Bain G, Conder G, Hine AL, Misra RR. Tuberculosis: A radiologic review. Radiographics. 2007;27:1255–73. - PubMed
-
- Craig WD, Wagner BJ, Travis MD. Pyelonephritis: Radiologic-pathologic review. Radiographics. 2008;28:255–77. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
