

Underutilization of cardiovascular medications: effect of a continuity-of-care program
- PMID: 23988600
- PMCID: PMC4019344
- DOI: 10.2146/ajhp120786
Underutilization of cardiovascular medications: effect of a continuity-of-care program
Abstract
Purpose: The effect of hospital pharmacists' enhanced communication with patients and community providers on the underutilization of key cardiovascular medications was studied.
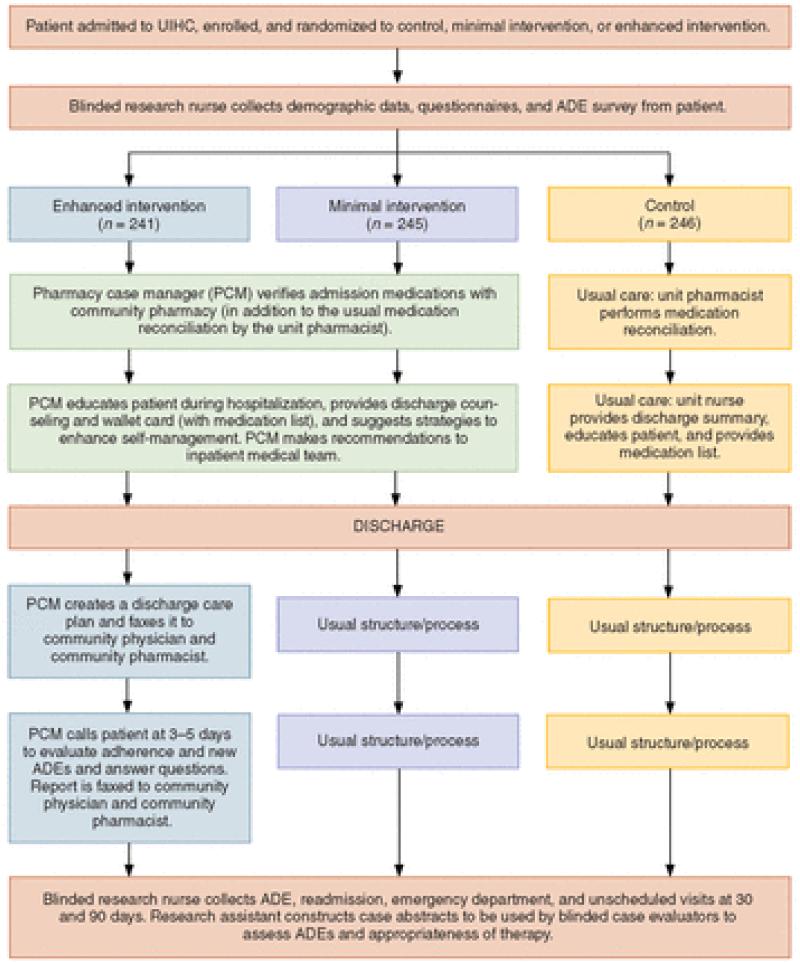
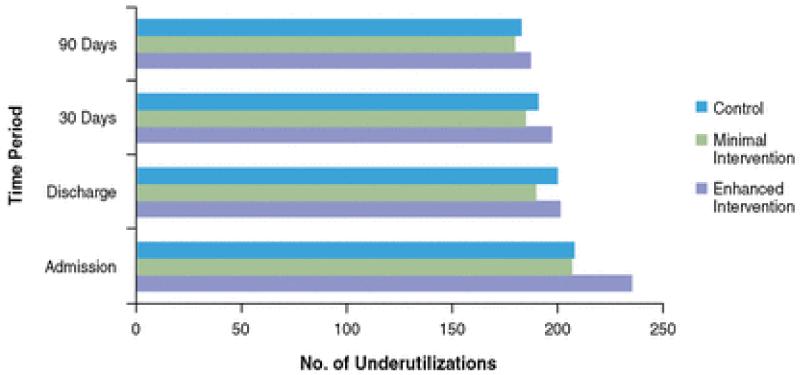
Methods: Patients enrolled in the Iowa Continuity of Care study were eligible for inclusion in this study if they had a diagnosis of hypertension, hyperlipidemia, heart failure, coronary artery disease, or a combination of these diagnoses. Eligible patients also had to be admitted to the internal medicine, family medicine, cardiology, or orthopedics services and receive their usual medical care in the community and their prescriptions from a community pharmacy. Patients were randomized to receive minimal intervention, enhanced intervention, or usual care. For the minimal- and enhanced-intervention groups, pharmacy case managers (PCMs) performed comprehensive medication reconciliations and identified drug-related problems within 24 hours of admission. The PCMs made recommendations to the inpatient care team and to patients' community physicians. For patients in the enhanced-intervention group, the PCM developed a discharge care plan containing the patient's discharge medication list. PCMs made specific recommendations to optimize regimens that did not meet current guidelines or medications that were underutilized. Medication underutilization was assessed at admission, discharge, 30 days after discharge, and 90 days after discharge.
Results: A total of 732 patients were enrolled in this study. There were no significant differences among the three study groups. Overall, the rate of underutilization remained constant among all three groups, despite enhanced pharmacist involvement in both intervention groups.
Conclusion: Enhanced interventions by PCMs had no effect on the underutilization of key cardiovascular drugs during hospitalization or after hospital discharge.
Figures
References
-
- Stafford RS, Radley DC. The underutilization of cardiac medications of proven benefit, 1990 to 2002. J Am Coll Cardiol. 2003;41:56–61. - PubMed
-
- Chobanian AV, Bakris GL, Black HR, et al. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension. 2003;42:1206–52. - PubMed
-
- Ong KL, Cheung BM, Man YB, et al. Prevalence, awareness, treatment, and control of hypertension among United States adults 1999-2004. Hypertension. 2007;49:69–75. - PubMed
-
- Kosecoff J, Kahn KL, Rogers WH, et al. Prospective payment system and impairment at discharge. The ‘quicker-and-sicker’ story revisited. JAMA. 1990;264:1980–3. - PubMed
-
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360:1418–28. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
