

Semiautomated volumetric measurement on postcontrast MR imaging for analysis of recurrent and residual disease in glioblastoma multiforme
- PMID: 23988756
- PMCID: PMC7964732
- DOI: 10.3174/ajnr.A3724
Semiautomated volumetric measurement on postcontrast MR imaging for analysis of recurrent and residual disease in glioblastoma multiforme
Abstract
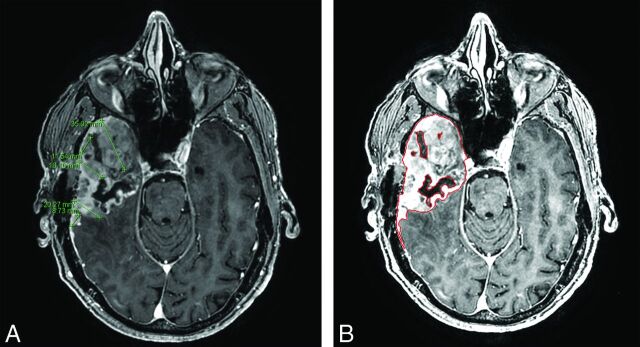
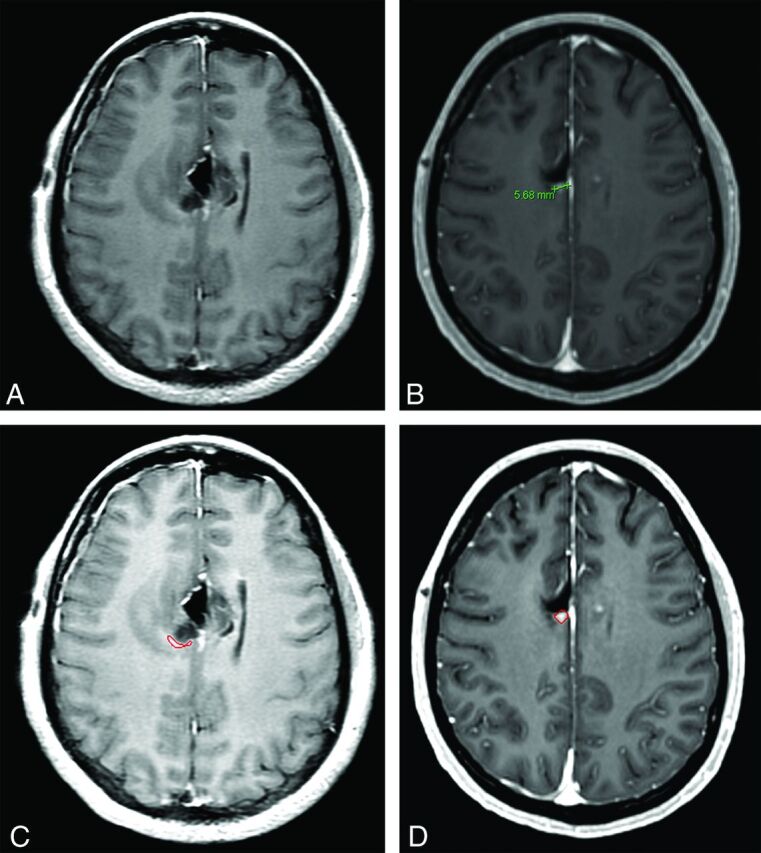
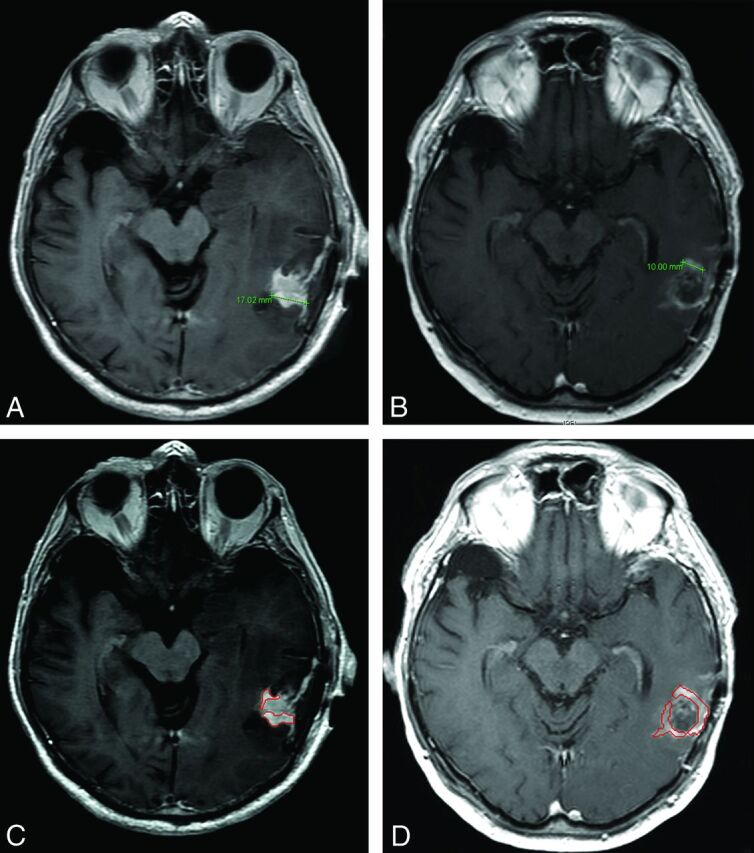
Background and purpose: A limitation in postoperative monitoring of patients with glioblastoma is the lack of objective measures to quantify residual and recurrent disease. Automated computer-assisted volumetric analysis of contrast-enhancing tissue represents a potential tool to aid the radiologist in following these patients. In this study, we hypothesize that computer-assisted volumetry will show increased precision and speed over conventional 1D and 2D techniques in assessing residual and/or recurrent tumor.
Materials and methods: This retrospective study included patients with native glioblastomas with MR imaging performed at 24-48 hours following resection and 2-4 months postoperatively. 1D and 2D measurements were performed by 2 neuroradiologists with Certificates of Added Qualification. Volumetry was performed by using manual segmentation and computer-assisted volumetry, which combines region-based active contours and a level set approach. Tumor response was assessed by using established 1D, 2D, and volumetric standards. Manual and computer-assisted volumetry segmentation times were compared. Interobserver correlation was determined among 1D, 2D, and volumetric techniques.
Results: Twenty-nine patients were analyzed. Discrepancy in disease status between 1D and 2D compared with computer-assisted volumetry was 10.3% (3/29) and 17.2% (5/29), respectively. The mean time for segmentation between manual and computer-assisted volumetry techniques was 9.7 minutes and <1 minute, respectively (P < .01). Interobserver correlation was highest for volumetric measurements (0.995; 95% CI, 0.990-0.997) compared with 1D (0.826; 95% CI, 0.695-0.904) and 2D (0.905; 95% CI, 0.828-0.948) measurements.
Conclusions: Computer-assisted volumetry provides a reproducible and faster volumetric assessment of enhancing tumor burden, which has implications for monitoring disease progression and quantification of tumor burden in treatment trials.
Figures
References
-
- Stupp R, Hegi ME, Mason WP, et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol 2009;10:459–66 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical