

Timing of limitations in life support in acute lung injury patients: a multisite study*
- PMID: 23989178
- PMCID: PMC3947055
- DOI: 10.1097/CCM.0b013e3182a272db
Timing of limitations in life support in acute lung injury patients: a multisite study*
Abstract
Objective: Substantial variability exists in the timing of limitations in life support for critically ill patients. Our objective was to investigate how the timing of limitations in life support varies with changes in organ failure status and time since acute lung injury onset.
Design, setting, and patients: This evaluation was performed as part of a prospective cohort study evaluating 490 consecutive acute lung injury patients recruited from 11 ICUs at three teaching hospitals in Baltimore, MD.
Interventions: None.
Measurements: The primary exposure was proportion of days without improvement in Sequential Organ Failure Assessment score, evaluated as a daily time-varying exposure. The outcome of interest was a documented limitation in life support defined as any of the following: 1) no cardiopulmonary resuscitation, 2) do not reintubate, 3) no vasopressors, 4) no hemodialysis, 5) do not escalate care, or 6) other limitations (e.g., "comfort care only").
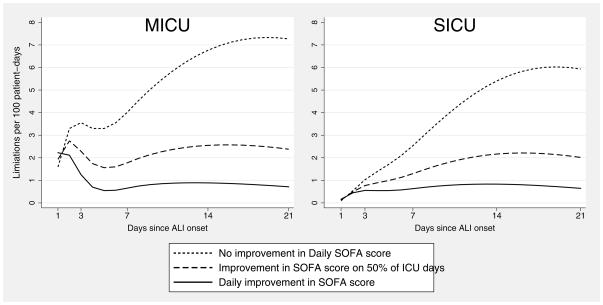
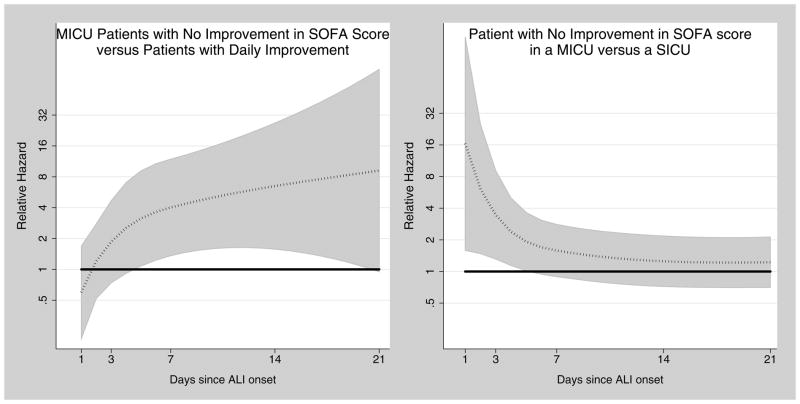
Main results: For medical ICU patients without improvement in daily Sequential Organ Failure Assessment score, the rate of limitation in life support tripled in the first 3 days after acute lung injury onset, increased again after day 5, and peaked at day 19. Compared with medical ICU patients, surgical ICU patients had a rate of limitations that was significantly lower during the first 5 days after acute lung injury onset. In all patients, more days without improvement in Sequential Organ Failure Assessment scores was associated with limitations in life support, independent of the absolute magnitude of the Sequential Organ Failure Assessment score.
Conclusions: Persistent organ failure is associated with an increase in the rate of limitations in life support independent of the absolute magnitude of Sequential Organ Failure Assessment score, and this association strengthens during the first weeks of treatment. During the first 5 days after acute lung injury onset, limitations were significantly more common in medical ICUs than surgical ICUs.
Conflict of interest statement
The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
Comment in
- Crit Care Med. 2014 Aug;42(8):e595-6
-
Clinical and economic implications of timing of limitations in life support.Crit Care Med. 2014 Feb;42(2):455-6. doi: 10.1097/CCM.0b013e3182a522de. Crit Care Med. 2014. PMID: 24434447 No abstract available.
-
Timing of limitations in the ICU and sequential organ failure assessment scores.Crit Care Med. 2014 Aug;42(8):e595-6. doi: 10.1097/CCM.0000000000000373. Crit Care Med. 2014. PMID: 25029149 No abstract available.
-
The authors reply.Crit Care Med. 2014 Aug;42(8):e596. doi: 10.1097/CCM.0000000000000447. Crit Care Med. 2014. PMID: 25029150 Free PMC article. No abstract available.
-
The authors reply.Crit Care Med. 2014 Aug;42(8):e596. Crit Care Med. 2014. PMID: 25674633 No abstract available.
-
Timing of limitations in the ICU and sequential organ failure assessment scores.Crit Care Med. 2014 Aug;42(8):e595-6. Crit Care Med. 2014. PMID: 27069986 No abstract available.
References
-
- Angus DC, Barnato AE, Linde-Zwirble WT, Weissfeld LA, Watson RS, Rickert T, Rubenfeld GD. Use of intensive care at the end of life in the United States: an epidemiologic study. Crit Care Med. 2004;32:638–643. - PubMed
-
- Prendergast TJ, Luce JM. Increasing incidence of withholding and withdrawal of life support from the critically ill. Am J Respir Crit Care Med. 1997;155:15–20. - PubMed
-
- Prendergast TJ, Claessens MT, Luce JM. A national survey of end-of-life care for critically ill patients. Am J Respir Crit Care Med. 1998;158:1163–1167. - PubMed
-
- Hall RI, Rocker GM. End-of-life care in the ICU: treatments provided when life support was or was not withdrawn. Chest. 2000;118:1424–1430. - PubMed
-
- Prendergast TJ, Puntillo KA. Withdrawal of life support: intensive caring at the end of life. Jama J Am Med Assoc. 2002;288:2732–2740. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
