

Review
doi: 10.2215/CJN.05810513.
Epub 2013 Aug 29.
Glomerular diseases: FSGS
Affiliations
- PMID: 23990165
- PMCID: PMC3944761
- DOI: 10.2215/CJN.05810513
Item in Clipboard
Review
Glomerular diseases: FSGS
Clin J Am Soc Nephrol.
2014 Mar.
Abstract
FSGS is a lesion, not a disease. The separation into primary FSGS (a result of immunologic-mediated injury) versus secondary FSGS (related to a variety of causes) is often difficult. Even when this particular issue is carefully evaluated, the therapeutic implications are not always apparent. Newer literature on both biomarker discovery and on the genetic basis of FSGS is reviewed in this context. In addition, the thorny implications of obesity as it relates to the FSGS lesion are discussed. An overall practical algorithmic approach to the management and treatment of the FSGS lesion that integrates these controversial overlap areas is suggested.
Figures
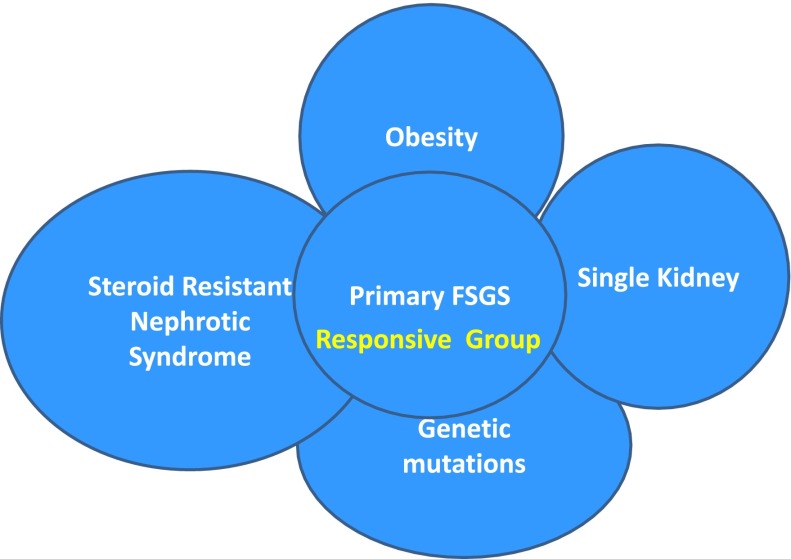
Overlap of different causal categories of FSGS. There is a complex interaction between different causes of FSGS. The overlap area conceptually indicates patients who may respond to treatment within the overlapping areas of primary and secondary causations.
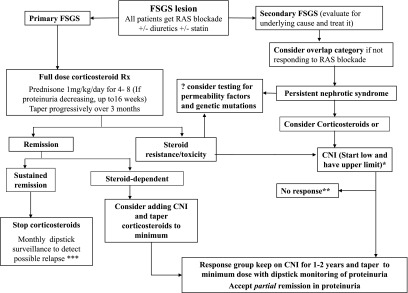
Treatment algorithm for FSGS. *CNI dose as per the KDIGO guidelines on GN. **See the text on options to consider in the management of nonresponders. ***See the text on how to manage relapse. RAS, renin-angiotensin system; CNI, calcineurin inhibitor; MMF, mycophenolate mofetil.
References
-
- Haas M, Meehan SM, Karrison TG, Spargo BH: Changing etiologies of unexplained adult nephrotic syndrome: A comparison of renal biopsy findings from 1976-1979 and 1995-1997. Am J Kidney Dis 30: 621–631, 1997 - PubMed
-
- Fuchshuber A, Gribouval O, Ronner V, Kroiss S, Karle S, Brandis M, Hildebrandt F: Clinical and genetic evaluation of familial steroid-responsive nephrotic syndrome in childhood. J Am Soc Nephrol 12: 374–378, 2001 - PubMed
-
- Hinkes B, Wiggins RC, Gbadegesin R, Vlangos CN, Seelow D, Nürnberg G, Garg P, Verma R, Chaib H, Hoskins BE, Ashraf S, Becker C, Hennies HC, Goyal M, Wharram BL, Schachter AD, Mudumana S, Drummond I, Kerjaschki D, Waldherr R, Dietrich A, Ozaltin F, Bakkaloglu A, Cleper R, Basel-Vanagaite L, Pohl M, Griebel M, Tsygin AN, Soylu A, Müller D, Sorli CS, Bunney TD, Katan M, Liu J, Attanasio M, O’toole JF, Hasselbacher K, Mucha B, Otto EA, Airik R, Kispert A, Kelley GG, Smrcka AV, Gudermann T, Holzman LB, Nürnberg P, Hildebrandt F: Positional cloning uncovers mutations in PLCE1 responsible for a nephrotic syndrome variant that may be reversible. Nat Genet 38: 1397–1405, 2006 - PubMed
-
- Kidney DiseaseImproving Global Outcomes (KDIGO) Glomerulonephritis Work Group: KDIGO Clinical Practice Guideline for Glomerulonephritis. Kidney Int Suppl 2: 139–274, 2012
-
- Korbet SM: Clinical picture and outcome of primary focal segmental glomerulosclerosis. Nephrol Dial Transplant 14[Suppl 3]: 68–73, 1999 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
