

Prevention of liver cancer cachexia-induced cardiac wasting and heart failure
- PMID: 23990596
- PMCID: PMC3977133
- DOI: 10.1093/eurheartj/eht302
Prevention of liver cancer cachexia-induced cardiac wasting and heart failure
Abstract
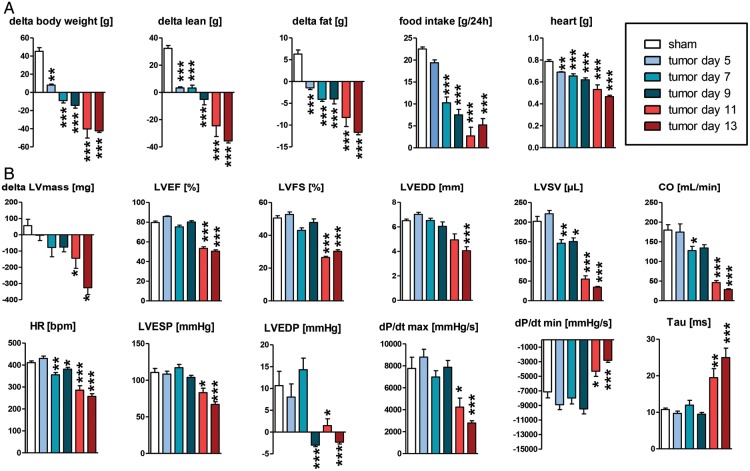
Aims: Symptoms of cancer cachexia (CC) include fatigue, shortness of breath, and impaired exercise capacity, which are also hallmark symptoms of heart failure (HF). Herein, we evaluate the effects of drugs commonly used to treat HF (bisoprolol, imidapril, spironolactone) on development of cardiac wasting, HF, and death in the rat hepatoma CC model (AH-130).
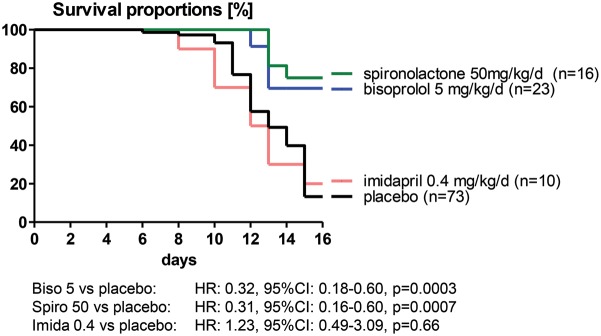
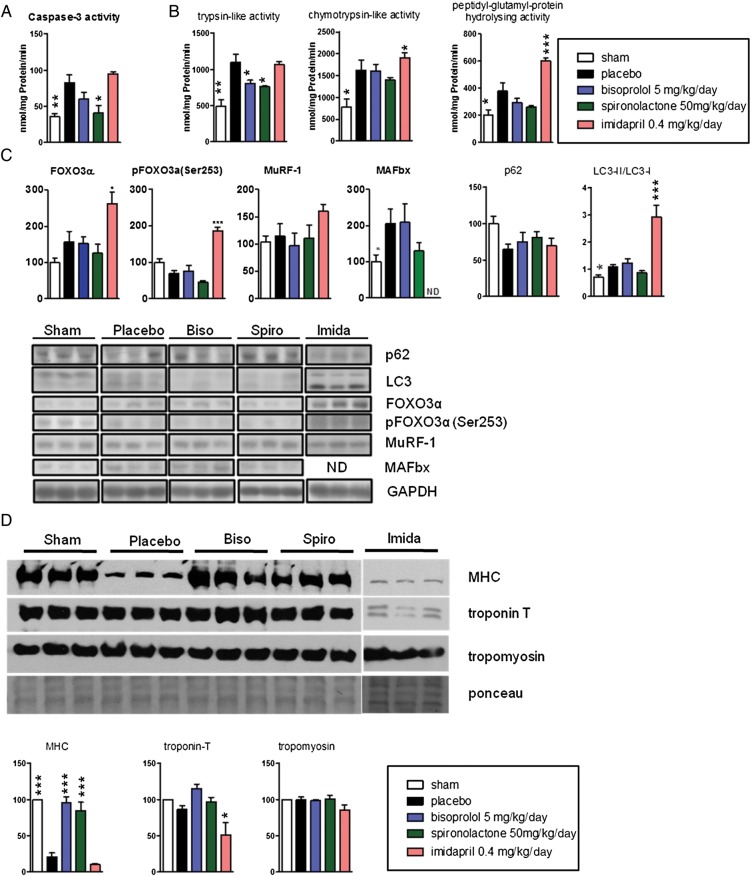
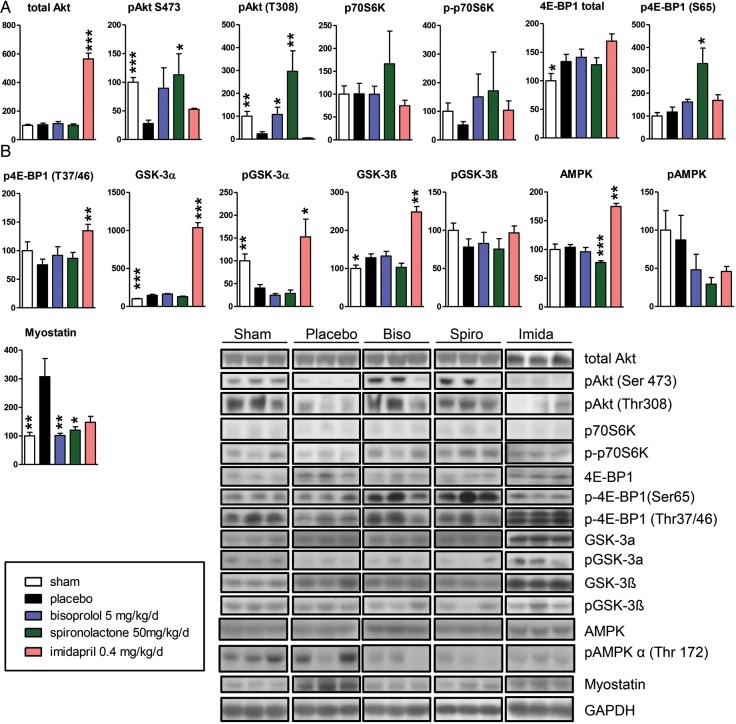
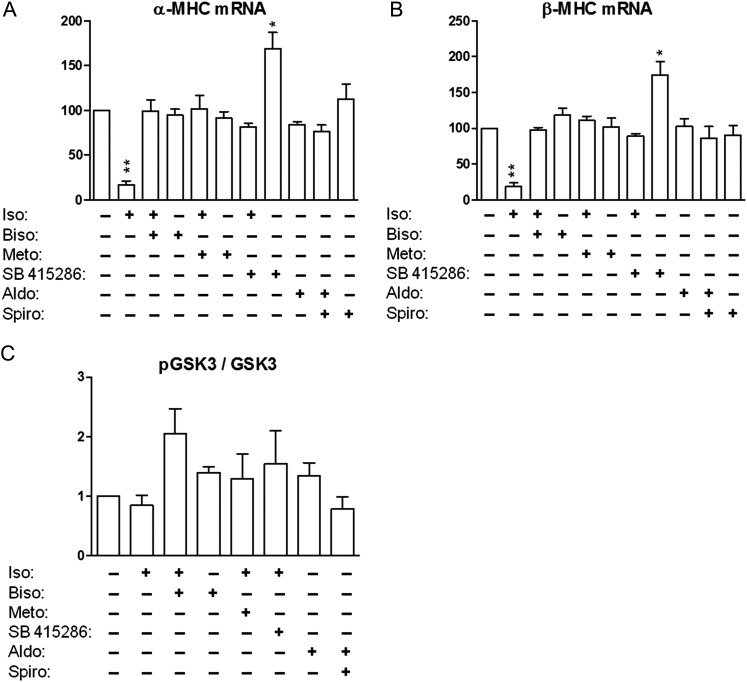
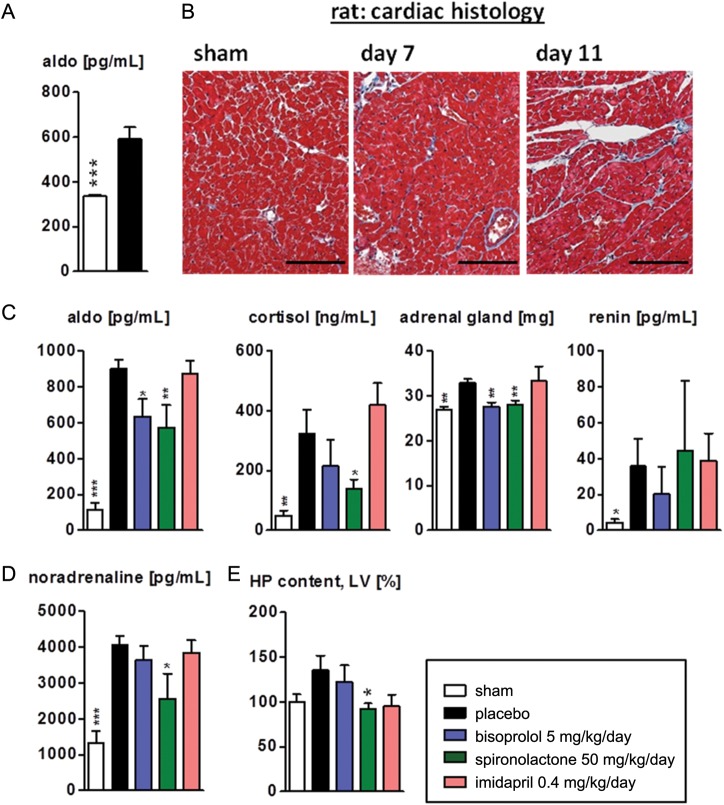
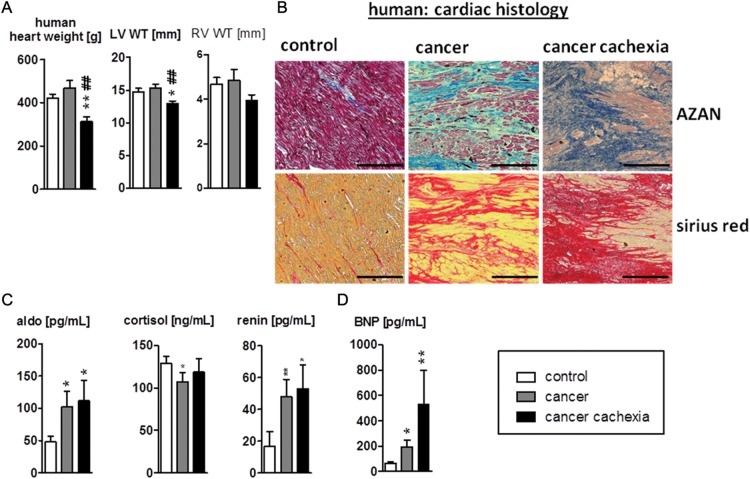
Methods and results: Tumour-bearing rats showed a progressive loss of body weight and left-ventricular (LV) mass that was associated with a progressive deterioration in cardiac function. Strikingly, bisoprolol and spironolactone significantly reduced wasting of LV mass, attenuated cardiac dysfunction, and improved survival. In contrast, imidapril had no beneficial effect. Several key anabolic and catabolic pathways were dysregulated in the cachectic hearts and, in addition, we found enhanced fibrosis that was corrected by treatment with spironolactone. Finally, we found cardiac wasting and fibrotic remodelling in patients who died as a result of CC. In living cancer patients, with and without cachexia, serum levels of brain natriuretic peptide and aldosterone were elevated.
Conclusion: Systemic effects of tumours lead not only to CC but also to cardiac wasting, associated with LV-dysfunction, fibrotic remodelling, and increased mortality. These adverse effects of the tumour on the heart and on survival can be mitigated by treatment with either the β-blocker bisoprolol or the aldosterone antagonist spironolactone. We suggest that clinical trials employing these agents be considered to attempt to limit this devastating complication of cancer.
Keywords: Cancer cachexia; Cardiac wasting; Heart failure; Intervention; Survival.
Figures
Comment in
-
Cancer cachexia: getting to the heart of the matter.Eur Heart J. 2019 Oct 21;40(40):e17-e19. doi: 10.1093/eurheartj/eht424. Eur Heart J. 2019. PMID: 24126874 Free PMC article. No abstract available.
References
-
- Garcia M, Jemal A, Ward EM, Center MM, Hao Y, Siegel RL, Thun MJ. Global Cancer Facts & Figures 2007. American Cancer Society 2007.
-
- Ahlberg K, Ekman T, Gaston-Johansson F, Mock V. Assessment and management of cancer-related fatigue in adults. Lancet. 2003;362:640–650. doi:10.1016/S0140-6736(03)14186-4. - DOI - PubMed
-
- Bruera E. ABC Of palliative care. Anorexia, cachexia, and nutrition. BMJ. 1997;315:1219–1222. doi:10.1136/bmj.315.7117.1219. - DOI - PMC - PubMed
-
- Tan BH, Fearon KC. Cachexia: prevalence and impact in medicine. Curr Opin Clin Nutr Metab Care. 2008;11:400–407. doi:10.1097/MCO.0b013e328300ecc1. - DOI - PubMed
-
- von Haehling S, Anker SD. Cachexia as a major underestimated and unmet medical need: facts and numbers. J Cachexia Sarcopenia Muscle. 2010;1:1–5. doi:10.1007/s13539-010-0002-6. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
