

Early PTSD symptom trajectories: persistence, recovery, and response to treatment: results from the Jerusalem Trauma Outreach and Prevention Study (J-TOPS)
- PMID: 23990895
- PMCID: PMC3750016
- DOI: 10.1371/journal.pone.0070084
Early PTSD symptom trajectories: persistence, recovery, and response to treatment: results from the Jerusalem Trauma Outreach and Prevention Study (J-TOPS)
Erratum in
- PLoS One. 2013;8(8). doi:10.1371/annotation/0af0b6c6-ac23-4fe9-a692-f5c30a3a30b3
Abstract
Context: Uncovering heterogeneities in the progression of early PTSD symptoms can improve our understanding of the disorder's pathogenesis and prophylaxis.
Objectives: To describe discrete symptom trajectories and examine their relevance for preventive interventions.
Design: Latent Growth Mixture Modeling (LGMM) of data from a randomized controlled study of early treatment. LGMM identifies latent longitudinal trajectories by exploring discrete mixture distributions underlying observable data.
Setting: Hadassah Hospital unselectively receives trauma survivors from Jerusalem and vicinity.
Participants: Adult survivors of potentially traumatic events consecutively admitted to the hospital's emergency department (ED) were assessed ten days and one-, five-, nine- and fifteen months after ED admission. Participants with data at ten days and at least two additional assessments (n = 957) were included; 125 received cognitive behavioral therapy (CBT) between one and nine months.
Approach: We used LGMM to identify latent parameters of symptom progression and tested the effect of CBT on these parameters. CBT consisted of 12 weekly sessions of either cognitive therapy (n = 41) or prolonged exposure (PE, n = 49), starting 29.8±5.7 days after ED admission, or delayed PE (n = 35) starting at 151.8±42.4 days. CBT effectively reduced PTSD symptoms in the entire sample.
Main outcome measure: Latent trajectories of PTSD symptoms; effects of CBT on these trajectories.
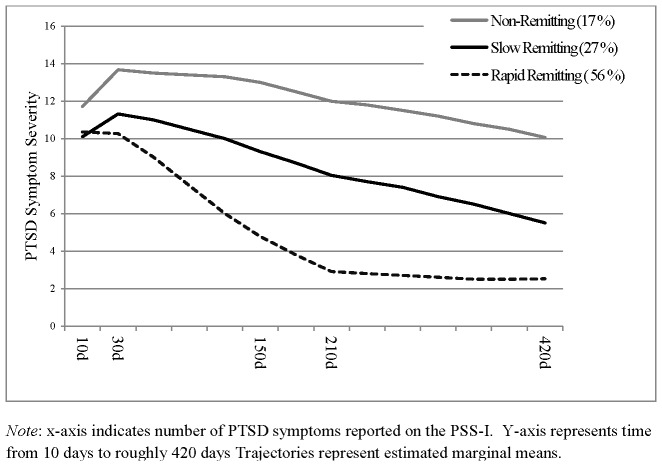
Results: THREE TRAJECTORIES WERE IDENTIFIED: Rapid Remitting (rapid decrease in symptoms from 1- to 5-months; 56% of the sample), Slow Remitting (progressive decrease in symptoms over 15 months; 27%) and Non-Remitting (persistently elevated symptoms; 17%). CBT accelerated the recovery of the Slow Remitting class but did not affect the other classes.
Conclusions: The early course of PTSD symptoms is characterized by distinct and diverging response patterns that are centrally relevant to understanding the disorder and preventing its occurrence. Studies of the pathogenesis of PTSD may benefit from using clustered symptom trajectories as their dependent variables.
Conflict of interest statement
Figures
References
-
- Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, et al. (2005) Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey replication. Arch Gen Psychiatry 62: 593–602. - PubMed
-
- Kessler RC (2000) Pmorosttraumatic stress disorder: the burden to the individual and to society. J Clin Psychiatry 61 Suppl 5: 4–12 discussion 13–14. - PubMed
-
- Kessler RC, Sonnega A, Bromet E, Hughes M, Nelson CB (1995) Posttraumatic stress disorder in the National Comorbidity Survey. Archives of General Psychiatry 52: 1048–1060. - PubMed
-
- Yehuda R, McFarlane AC, Shalev AY (1998) Predicting the development of posttraumatic stress disorder from the acute response to a traumatic event. Biological Psychiatry 44: 1305–1313. - PubMed
-
- Koren D, Arnon I, Klein E (2001) Long term course of chronic posttraumatic stress disorder in traffic accident victims: a three-year prospective follow-up study. Behav Res Ther 39: 1449–1458. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
