

Risk factors for acute endophthalmitis following cataract surgery: a systematic review and meta-analysis
- PMID: 23990980
- PMCID: PMC3753305
- DOI: 10.1371/journal.pone.0071731
Risk factors for acute endophthalmitis following cataract surgery: a systematic review and meta-analysis
Abstract
Background: Acute endophthalmitis is one of the most serious complications of cataract surgery and often results in severe visual impairment. Several risk factors for acute postoperative endophthalmitis (POE) following cataract surgery have been reported but the level of evidence and strength of association is varied. The purpose of this study was to critically appraise published reports on and to summarize clinical risk factors associated with acute POE which could be easily assessed by ophthalmologists for the introduction and implementation of preventive measure.
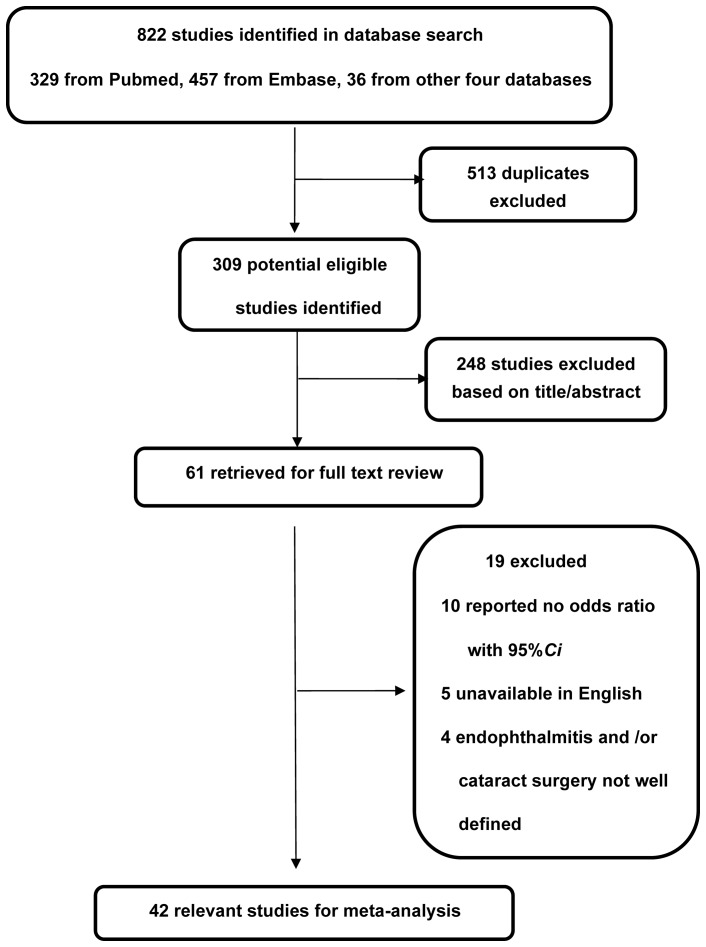
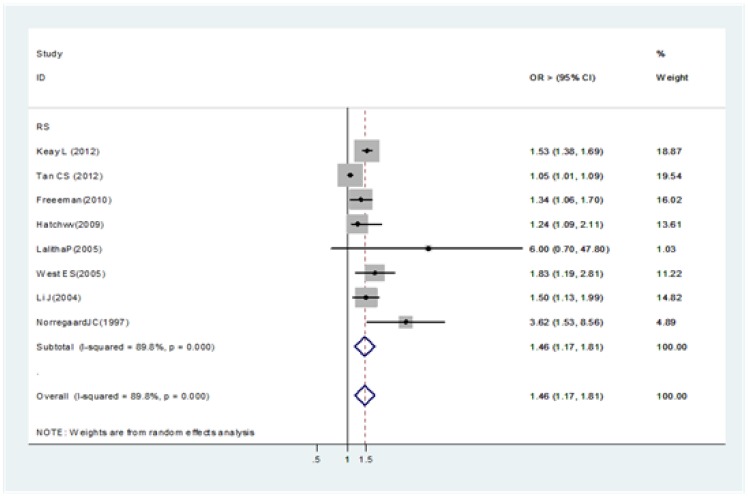
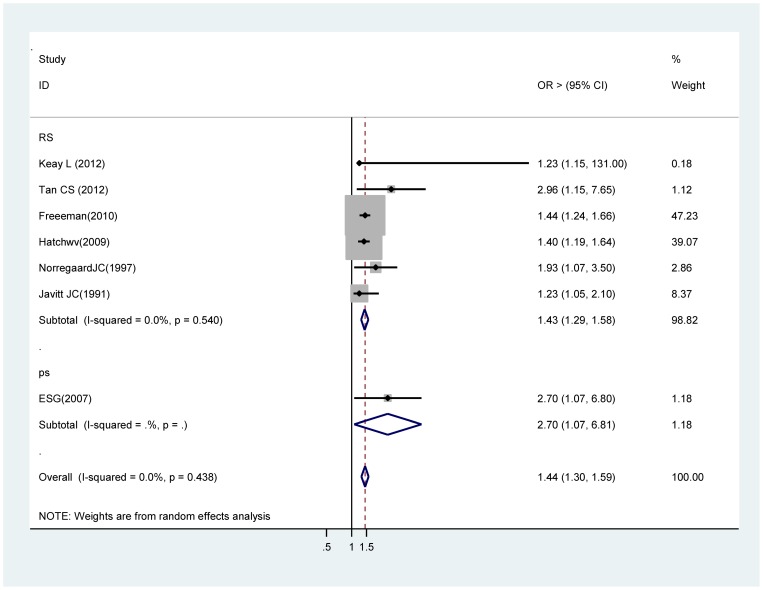
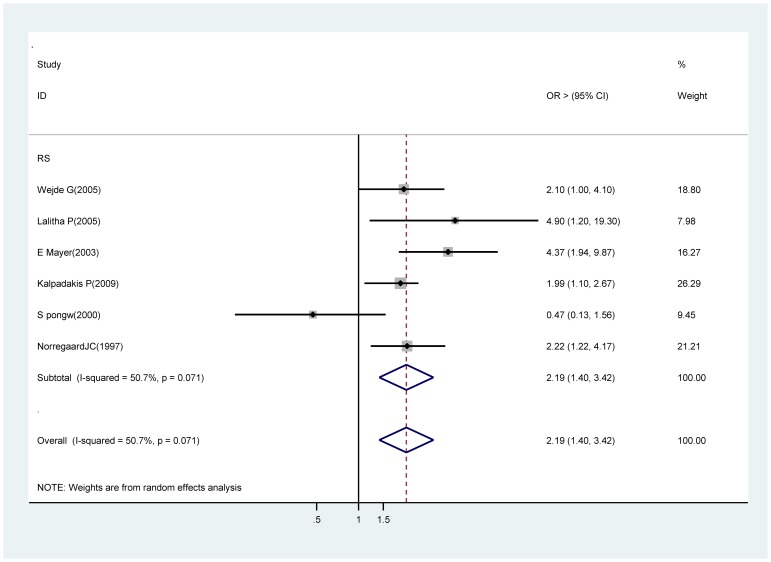
Methods: A systematic review and meta-analysis of observational studies was performed. Six databases were searched with no limits on the year or language of publication. Study-specific odds ratios (Ors) or relative risk (RR) of each risk factor were pooled using a random effect model.
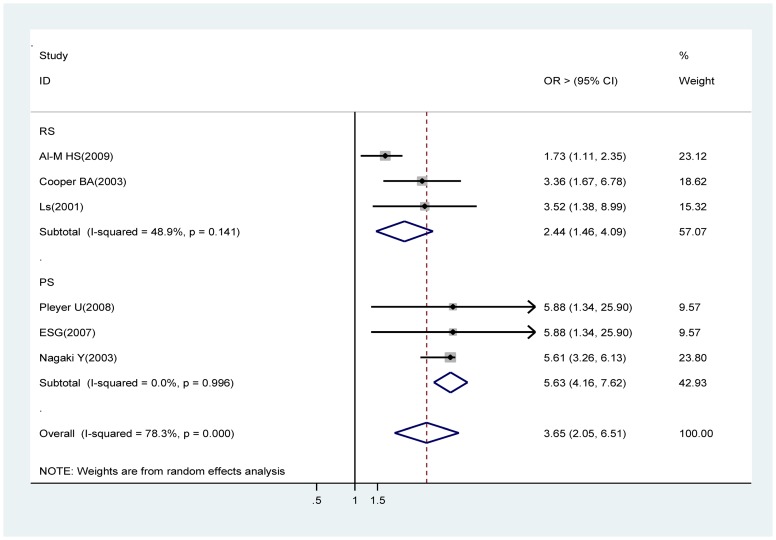
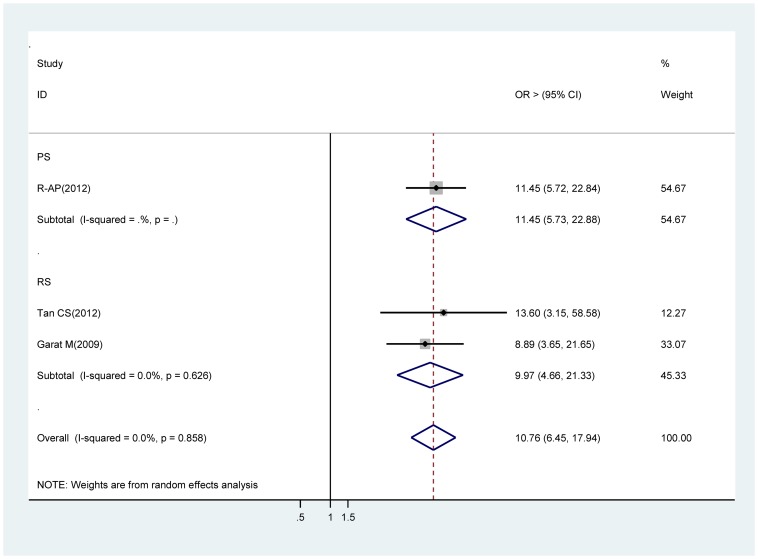
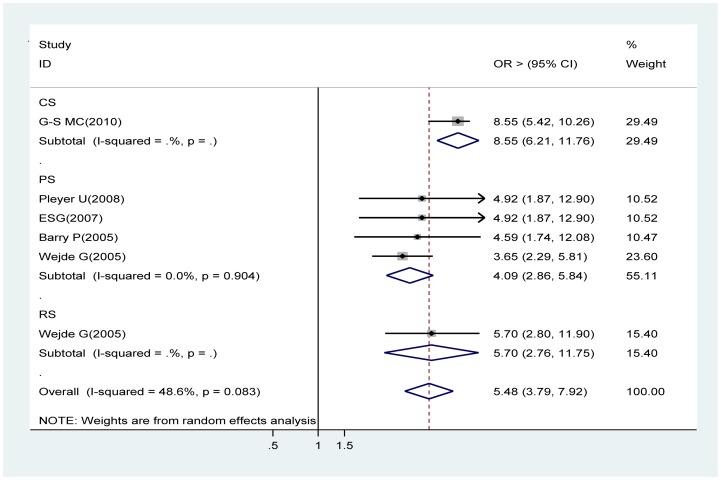
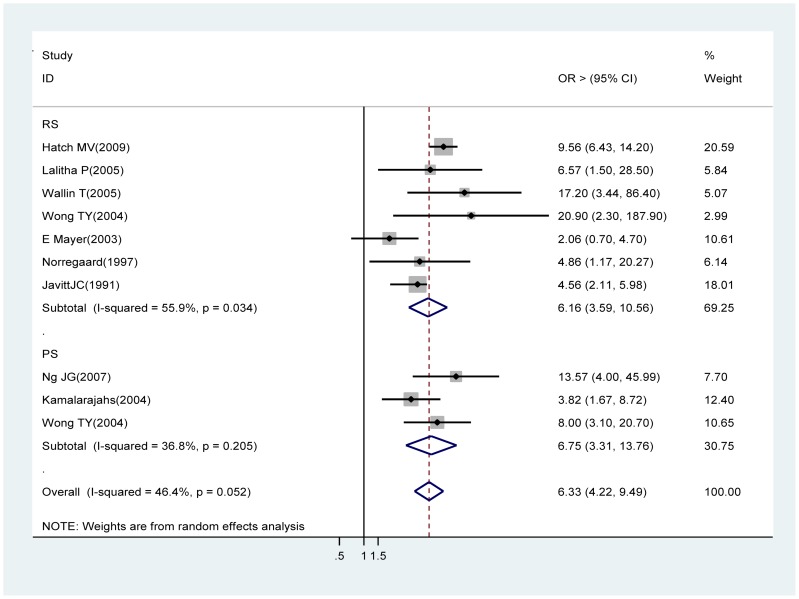
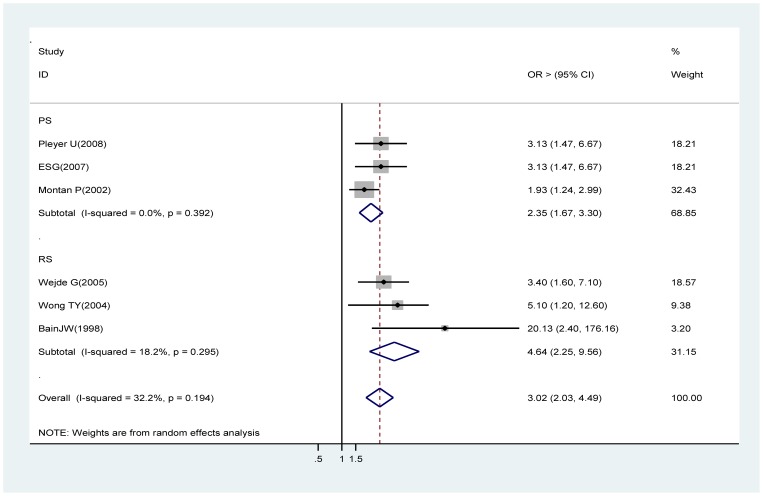
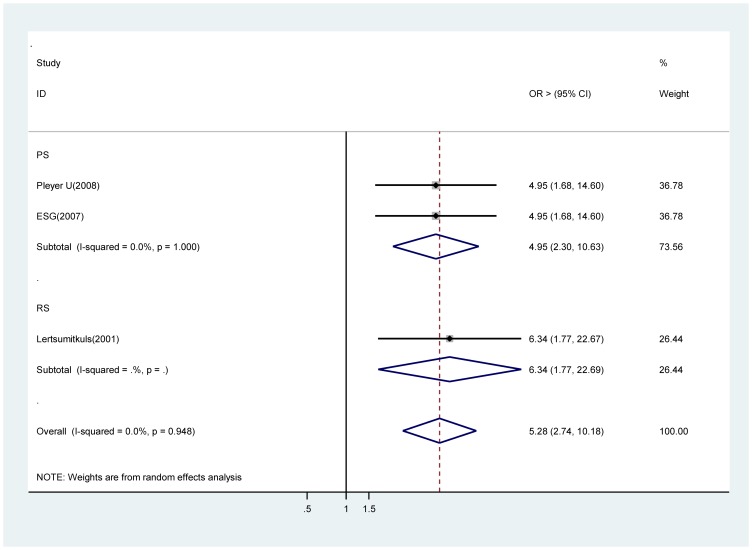
Results: A total of 6 686 169 participants with 8 963 endophthalmitis in 42 studies were analyzed. Of the nine risk factors identified in our systematic review and meta-analysis, extra- or intracapsular cataract extraction, a clear corneal incision, without intracameral cefazolin (1 mg in 0.1 ml solution), without intracameral cefuroxime (1 mg in 0.1 ml solution), post capsular rupture, silicone intraocular lenses and intraoperative complications were found strongly associated with acute endophthalmitis. Other significant factors with a lower strength of association (risk estimates generally 1.5 or less) were male gender and old age (85 years and older).
Conclusions: Our study provides summary data on the risk factors for acute POE. Identifying patients at high risk of this sight-threatening eye disease is important from both the public health and clinical perspectives as this would facilitate detection of disease before the onset of irreversible visual loss enabling earlier intervention.
Conflict of interest statement
Figures
References
-
- World Health Organization. (2012) Blindness. Available at: http://www.who.int/blindness/en/.
-
- Ng JQ, Morlet N, Pearman JW, Constable IJ, McAllister IL, et al. (2005) Management and outcomes of postoperative endophthalmitis since the Endophthalmitis Vitrectomy Study: the Endophthalmitis Population Study of Western Australia (EPSWA) 's fifth report. Ophthalmology 112: 1199–1206. - PubMed
-
- Taban M, Behrens A, Newcomb RL, Nobe MY, Saedi G, et al. (2005) Acute endophthalmitis following cataract surgery: a systematic review of the literature. Arch Ophthalmol 123: 613–620. - PubMed
-
- Yu CQ, Ta CN (2012) Prevention of postcataract endophthalmitis: evidence-based medicine. Curr Opin Ophthalmol 23(1): 19–25. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
