

Neonatal intensive care in a Karen refugee camp: a 4 year descriptive study
- PMID: 23991145
- PMCID: PMC3749980
- DOI: 10.1371/journal.pone.0072721
Neonatal intensive care in a Karen refugee camp: a 4 year descriptive study
Abstract
Background: A third of all deaths in children aged <5 years occur in the neonatal period. Neonatal intensive care is often considered too complex and expensive to be implemented in resource poor settings. Consequently the reductions that have been made in infant mortality in the poorest countries have not been made in the neonatal period. This manuscript describes the activities surrounding the introduction of special care baby unit (SCBU) in a refugee setting and the resulting population impact.
Methods: A SCBU was developed in Maela refugee camp on the Thailand-Myanmar border. This unit comprised of a dedicated area, basic equipment, drugs and staff training. Training was built around neonatal guidelines, comprising six clinical steps: recognition, resuscitation, examination, supportive medical care, specialised medical care, and counselling of parents with sick newborns.
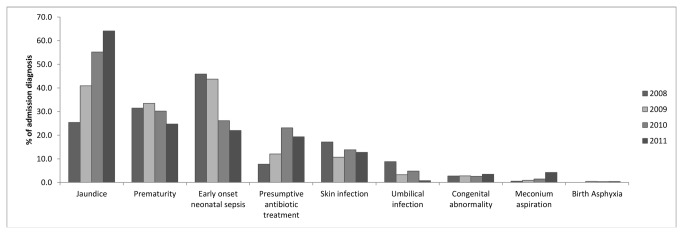
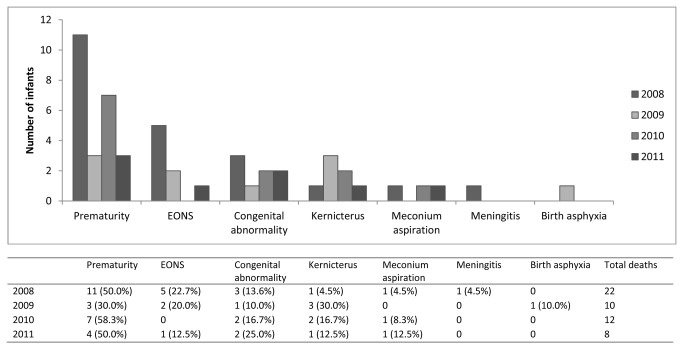
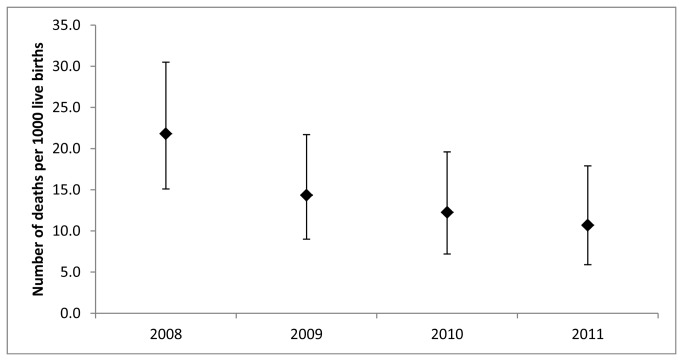
Results: From January 2008 until December 2011, 952 infants were admitted to SCBU. The main admission diagnoses were early onset neonatal sepsis, jaundice and prematurity. Early prematurity (<34 weeks) carried the highest risk of mortality (OR 9.5, 95% CI 5.4-16.5, p<0.001). There was a significant decrease in mortality from 19.3% (2008) to 4.8% (2011) among the infants admitted for prematurity (p=0.03). The neonatal mortality in Maela camp as a whole declined by 51% from 21.8 to 10.7 deaths per 1000 live births over the corresponding period (p=0.04). Staff expressed more confidence in their ability to take care of neonates and there was a more positive attitude towards premature infants.
Conclusion: Neonatal mortality can be reduced in a resource poor setting by introduction of a simple low cost unit specialising in care of sick neonates and run by local health workers following adequate training. Training in recognition and provision of simple interventions at a high standard can increase staff confidence and reduce fatalistic attitudes towards premature neonates.
Conflict of interest statement
Figures
Comment in
-
The profile of a life-saving researcher.Educ Prim Care. 2018 Mar;29(2):113-114. doi: 10.1080/14739879.2018.1437570. Epub 2018 Feb 15. Educ Prim Care. 2018. PMID: 29447583
References
-
- Liu L, Johnson HL, Cousens S, Perin J, Scott S et al. (2012) Global, regional, and national causes of child mortality: an updated systematic analysis for 2010 with time trends since 2000. Lancet 379: 2151-2161. doi:10.1016/S0140-6736(12)60560-1. PubMed: 22579125. - DOI - PubMed
-
- Lawn JE, Cousens S, Zupan J (2005) 4 million neonatal deaths: when? Where? Why? Lancet 365: 891-900. doi:10.1016/S0140-6736(05)71048-5. PubMed: 15752534. - DOI - PubMed
-
- Black RE, Morris SS, Bryce J (2003) Where and why are 10 million children dying every year? Lancet 361: 2226-2234. doi:10.1016/S0140-6736(03)13779-8. PubMed: 12842379. - DOI - PubMed
-
- Black RE, Cousens S, Johnson HL, Lawn JE, Rudan I et al. (2010) Global, regional, and national causes of child mortality in 2008: a systematic analysis. Lancet 375: 1969-1987. doi:10.1016/S0140-6736(10)60549-1. PubMed: 20466419. - DOI - PubMed
-
- Amouzou A, Habi O, Bensaïd K (2012) Reduction in child mortality in Niger: a Countdown to 2015 country case study. Lancet 380: 1169-1178. doi:10.1016/S0140-6736(12)61376-2. PubMed: 22999428. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
