

Pancreatic neuroendocrine tumours: hypoenhancement on arterial phase computed tomography predicts biological aggressiveness
- PMID: 23991643
- PMCID: PMC3967881
- DOI: 10.1111/hpb.12139
Pancreatic neuroendocrine tumours: hypoenhancement on arterial phase computed tomography predicts biological aggressiveness
Abstract
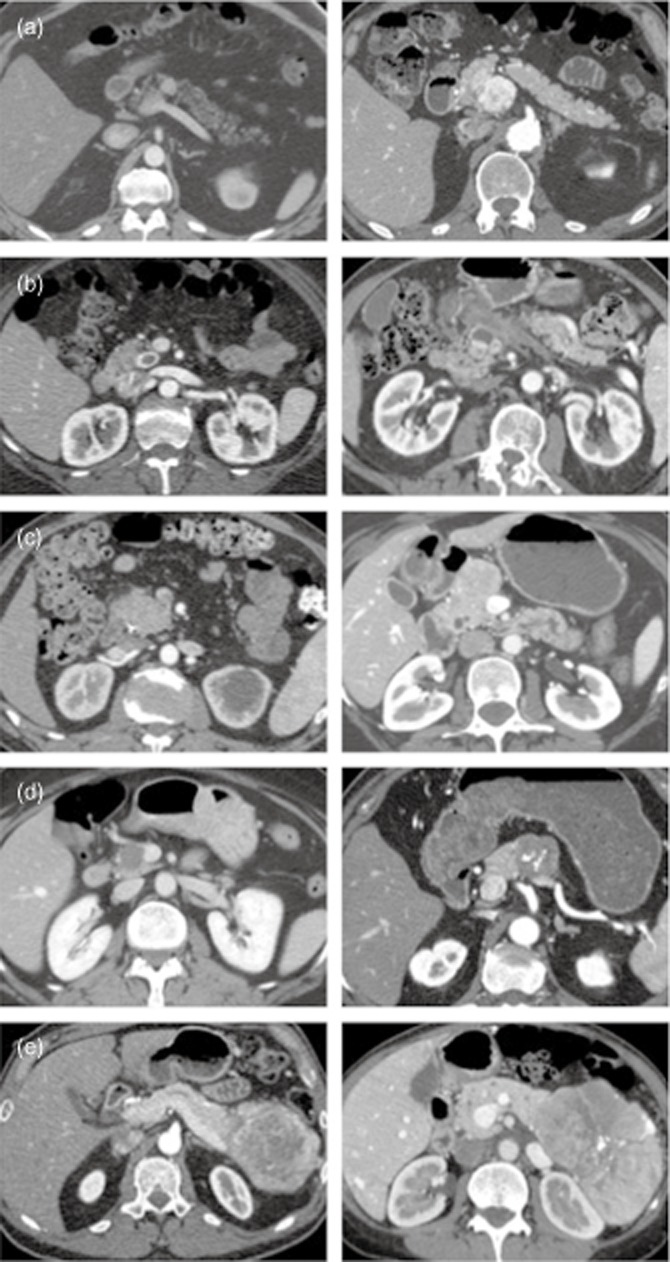
Background: Contrary to pancreatic adenocarcinoma, pancreatic neuroendocrine tumours (PNET) are commonly hyperenhancing on arterial phase computed tomography (APCT). However, a subset of these tumours can be hypoenhancing. The prognostic significance of the CT appearance of these tumors remains unclear.
Methods: From 2001 to 2012, 146 patients with well-differentiated PNET underwent surgical resection. The degree of tumour enhancement on APCT was recorded and correlated with clinicopathological variables and overall survival.
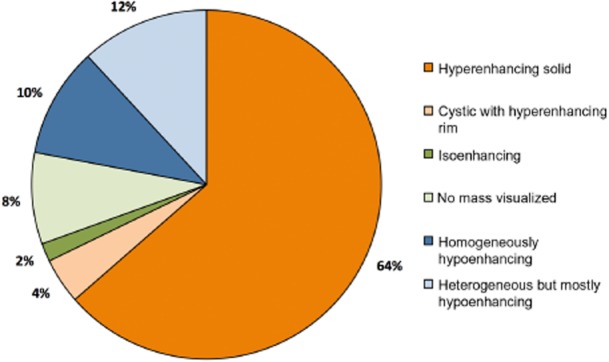
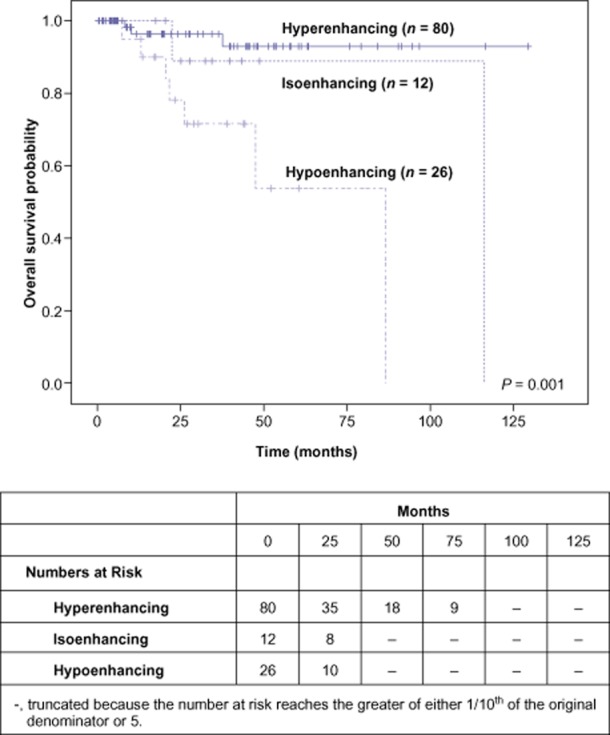
Results: APCT images were available for re-review in 118 patients (81%). The majority had hyperenhancing tumours (n = 80, 68%), 12 (10%) were isoenhancing (including cases where no mass was visualized) and 26 (22%) were hypoenhancing. Hypoenhancing PNET were larger, more commonly intermediate grade, and had higher rates of lymph node and synchronous liver metastases. Hypoenhancing PNET were also associated with significantly worse overall survival after a resection as opposed to isoenhancing and hyperenhancing tumours (5-year, 54% versus 89% versus 93%). On multivariate analysis of factors available pre-operatively, only hypoenhancement (HR 2.32, P = 0.02) was independently associated with survival.
Discussion: Hypoenhancement on APCT was noted in 22% of well-differentiated PNET and was an independent predictor of poor outcome. This information can inform pre-operative decisions in the multidisciplinary treatment of these neoplasms.
© 2013 International Hepato-Pancreato-Biliary Association.
Figures
References
-
- Klimstra DS, Modlin IR, Coppola D, Lloyd RV, Suster S. The pathologic classification of neuroendocrine tumors: a review of nomenclature, grading, and staging systems. Pancreas. 2010;39:707–712. - PubMed
-
- Fitzgerald TL, Hickner ZJ, Schmitz M, Kort EJ. Changing incidence of pancreatic neoplasms: a 16-year review of statewide tumor registry. Pancreas. 2008;37:134–138. - PubMed
-
- Caldarella A, Crocetti E, Paci E. Distribution, incidence, and prognosis in neuroendocrine tumors: a population based study from a cancer registry. Pathol Oncol Res. 2011;17:759–763. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
