

Characterization of symptoms in irritable bowel syndrome with mixed bowel habit pattern
- PMID: 23991913
- PMCID: PMC3865067
- DOI: 10.1111/nmo.12220
Characterization of symptoms in irritable bowel syndrome with mixed bowel habit pattern
Abstract
Background: Irritable bowel syndrome (IBS) with mixed bowel habits (IBS-M) is a heterogeneous subtype with varying symptoms of constipation and diarrhea, and has not been well characterized. We aimed to characterize gastrointestinal (GI) and non-GI symptoms in IBS-M patients from a US patient population, and to compare them with IBS with constipation (IBS-C) and diarrhea (IBS-D).
Methods: Subjects answering community advertisements and meeting Rome III criteria for IBS completed symptom questionnaires.
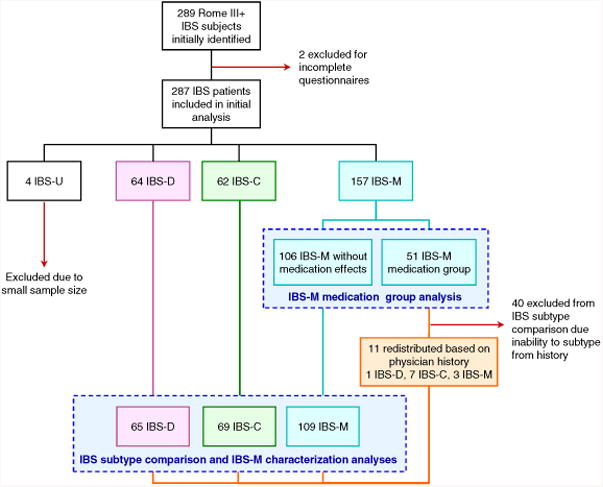
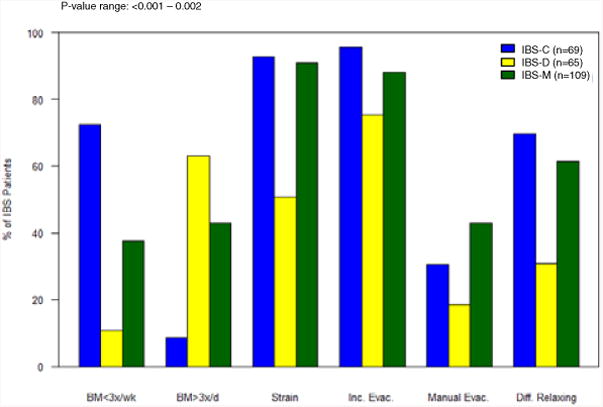
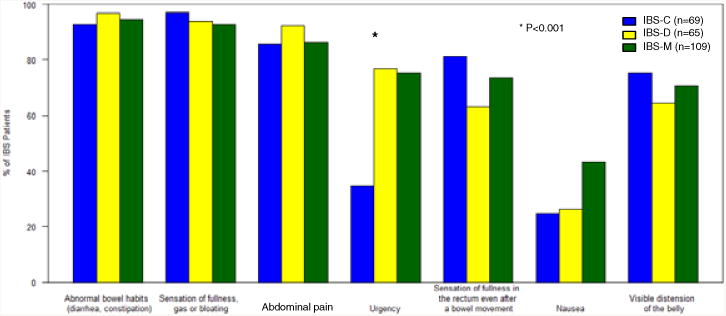
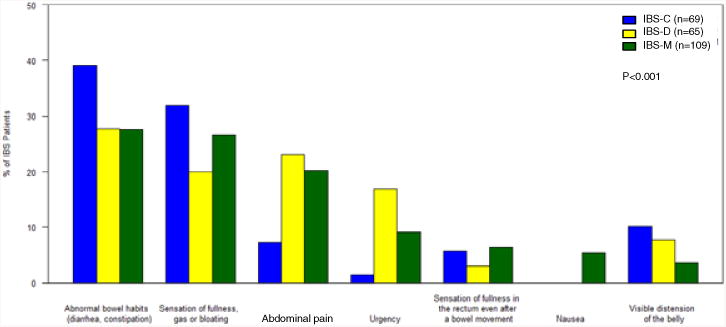
Key results: Of the initial 289 IBS patients identified, one third (n = 51, 32.5%) who met Rome III criteria for IBS-M endorsed having either loose stools or hard stools due to medication. These patients had more severe symptoms and longer duration of flares compared to the rest of the IBS-M group (p = 0.014, p = 0.005). Excluding IBS-M patients with medication-related extremes in stool form who could not be reclassified by medical history, 247 IBS patients were assessed. IBS-M was the most common (44.1%), followed by IBS-C (27.9%), IBS-D (26.3%), and IBS-U (unsubtyped, 1.6%). While IBS-M shared symptoms with both IBS-C and IBS-D, there were significant differences in the prevalence of bowel habit symptoms (p-value range: <0.001-0.002). IBS-M patients reported most bothersome symptoms that were more similar to IBS-D, with the most common being irregular bowel habits (27.5%), bloating (26.6%), and abdominal pain (20.2%). There were no differences in non-GI symptoms between subtypes.
Conclusions & inferences: IBS-M is a heterogeneous symptom group and thus requires that subclassification criteria be better defined. Use of laxative/antidiarrheal medications adds to the diagnostic complexity in a potentially more severe subset of IBS-M and should be assessed for accurate subclassification.
Keywords: abdominal pain; constipation; diarrhea; irritable bowel syndrome; mixed bowel habits.
© 2013 John Wiley & Sons Ltd.
Conflict of interest statement
Figures
Comment in
-
Irritable bowel syndrome subtypes: constipation, diarrhea…and mixed bowel pattern: tertium datur.Neurogastroenterol Motil. 2014 Jan;26(1):1-2. doi: 10.1111/nmo.12274. Neurogastroenterol Motil. 2014. PMID: 24329945
References
-
- Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, Spiller RC. Functional bowel disorders. Gastroenterology. 2006 Apr;130(5):1480–91. Epub 2006/05/09. eng. - PubMed
-
- Drossman DA, Morris CB, Hu Y, Toner BB, Diamant N, Leserman J, et al. A prospective assessment of bowel habit in irritable bowel syndrome in women: defining an alternator. Gastroenterology. 2005 Mar;128(3):580–9. Epub 2005/03/15. eng. - PubMed
-
- Mearin F, Balboa A, Badia X, Baro E, Caldwell E, Cucala M, et al. Irritable bowel syndrome subtypes according to bowel habit: revisiting the alternating subtype. Eur J Gastroenterol Hepatol. 2003 Feb;15(2):165–72. Epub 2003/02/01. eng. - PubMed
-
- Hungin AP, Whorwell PJ, Tack J, Mearin F. The prevalence, patterns and impact of irritable bowel syndrome: an international survey of 40,000 subjects. Aliment Pharmacol Ther. 2003 Mar 1;17(5):643–50. Epub 2003/03/19. eng. - PubMed
-
- Spiller RC, Meyers NL, Hickling RI. Identification of patients with non-d, non-C irritable bowel syndrome and treatment with renzapride: an exploratory, multicenter, randomized, double-blind, placebo-controlled clinical trial. Dig Dis Sci. 2008 Dec;53(12):3191–200. Epub 2008/05/10. eng. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
