

Reduction of breast cancer relapses with perioperative non-steroidal anti-inflammatory drugs: new findings and a review
- PMID: 23992307
- PMCID: PMC3831877
- DOI: 10.2174/09298673113209990250
Reduction of breast cancer relapses with perioperative non-steroidal anti-inflammatory drugs: new findings and a review
Abstract
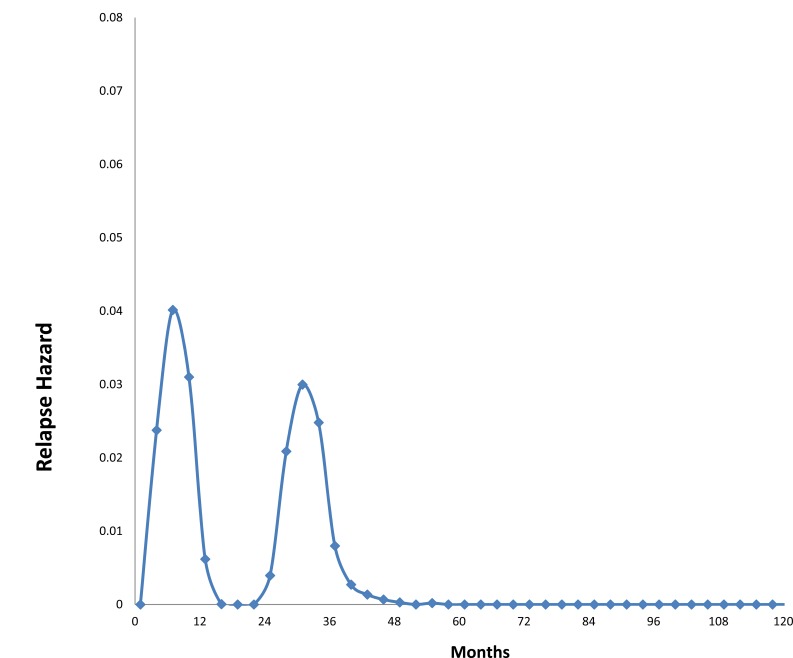
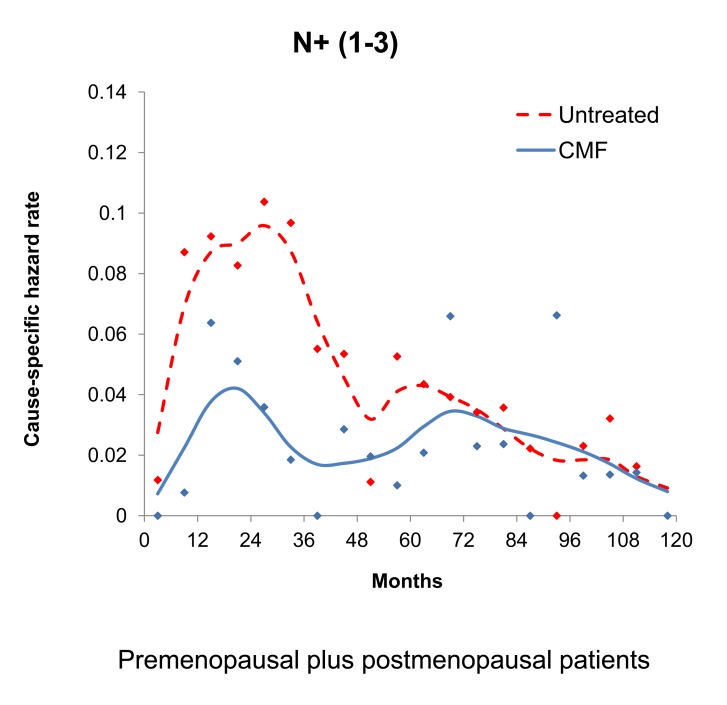
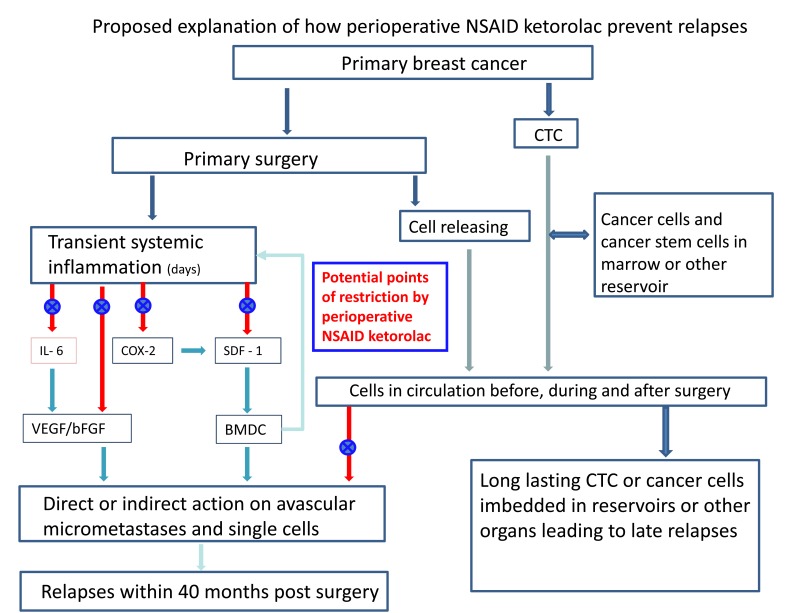
To explain a bimodal pattern of hazard of relapse among early stage breast cancer patients identified in multiple databases, we proposed that late relapses result from steady stochastic progressions from single dormant malignant cells to avascular micrometastases and then on to growing deposits. However in order to explain early relapses, we had to postulate that something happens at about the time of surgery to provoke sudden exits from dormant phases to active growth and then to detection. Most relapses in breast cancer are in the early category. Recent data from Forget et al. suggest an unexpected mechanism. They retrospectively studied results from 327 consecutive breast cancer patients comparing various perioperative analgesics and anesthetics in one Belgian hospital and one surgeon. Patients were treated with mastectomy and conventional adjuvant therapy. Relapse hazard updated Sept 2011 are presented. A common Non-Steroidal Anti-Inflammatory Drug (NSAID) analgesic used in surgery produced far superior disease-free survival in the first 5 years after surgery. The expected prominent early relapse events in months 9-18 are reduced 5-fold. If this observation holds up to further scrutiny, it could mean that the simple use of this safe, inexpensive and effective anti-inflammatory agent at surgery might eliminate early relapses. Transient systemic inflammation accompanying surgery could facilitate angiogenesis of dormant micrometastases, proliferation of dormant single cells, and seeding of circulating cancer stem cells (perhaps in part released from bone marrow) resulting in early relapse and could have been effectively blocked by the perioperative anti-inflammatory agent.
Figures







References
-
- Popper KR. The Logic of Scientific Discovery, (revised) London: Hutchinson & Co; 1968.
-
- Kuhn TS. The Structure of Scientific Revolution. Second Edition, Enlarged. Chicago: The University of Chicago Press; 1970(1962).
-
- Ariel I. A historical review of breast cancer treatment. In: Leslie W, Houston J, editors. Breast Cancer: Controversies in Management. Armonk, NY: Futura Publishing Co; 1994.
-
- Virchow R. Die Krankhaften Geschwulste. Vol. 1. Berlin: Hirshwald Publishers; pp. 1863–1873.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
