

Outgrowth of the bacterial airway microbiome after rhinovirus exacerbation of chronic obstructive pulmonary disease
- PMID: 23992479
- PMCID: PMC3863728
- DOI: 10.1164/rccm.201302-0341OC
Outgrowth of the bacterial airway microbiome after rhinovirus exacerbation of chronic obstructive pulmonary disease
Abstract
Rationale: Rhinovirus infection is followed by significantly increased frequencies of positive, potentially pathogenic sputum cultures in chronic obstructive pulmonary disease (COPD). However, it remains unclear whether these represent de novo infections or an increased load of organisms from the complex microbial communities (microbiome) in the lower airways.
Objectives: To investigate the effect of rhinovirus infection on the airway bacterial microbiome.
Methods: Subjects with COPD (n = 14) and healthy control subjects with normal lung function (n = 17) were infected with rhinovirus. Induced sputum was collected at baseline before rhinovirus inoculation and again on Days 5, 15, and 42 after rhinovirus infection and DNA was extracted. The V3-V5 region of the bacterial 16S ribosomal RNA gene was amplified and pyrosequenced, resulting in 370,849 high-quality reads from 112 of the possible 124 time points.
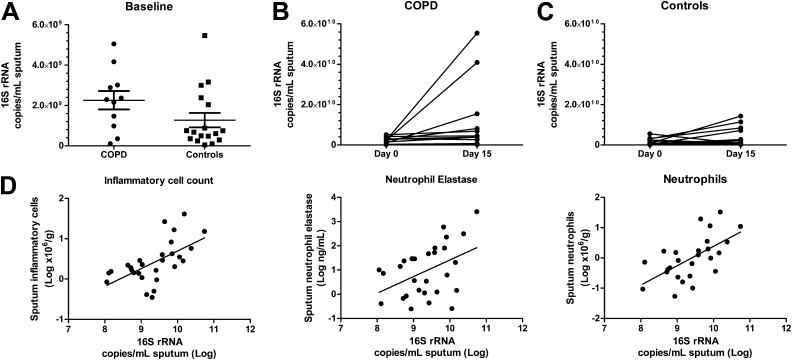
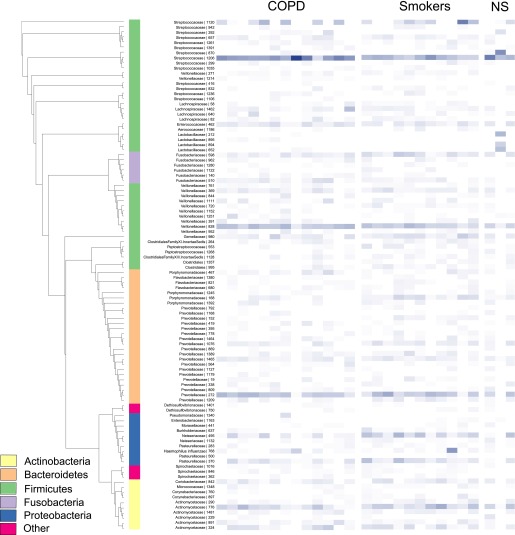
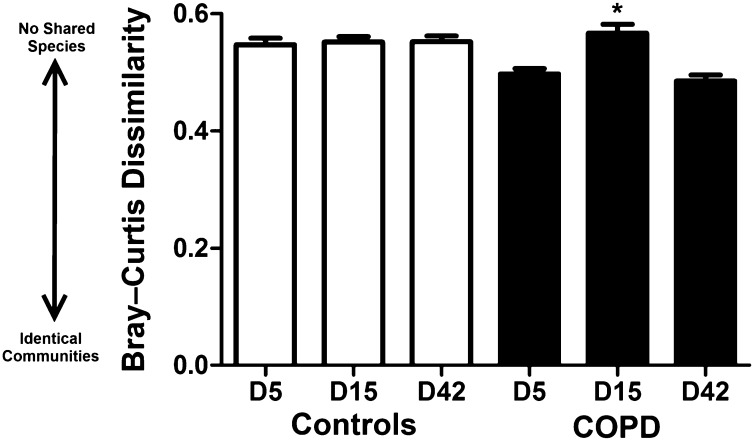
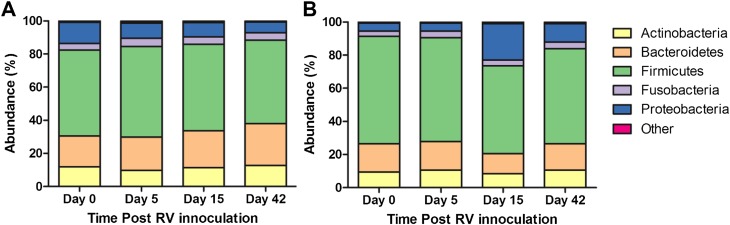
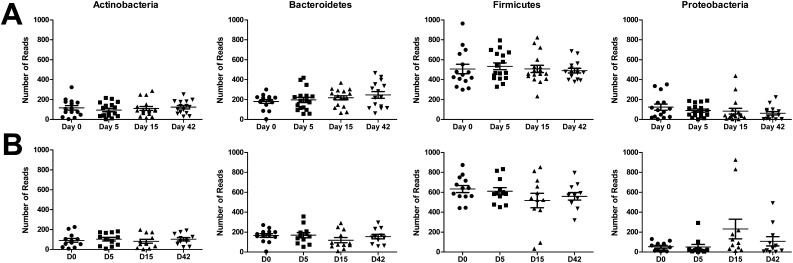
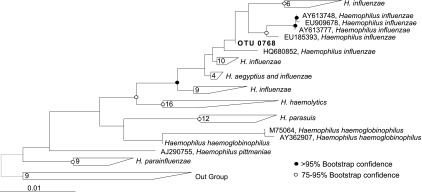
Measurements and main results: At 15 days after rhinovirus infection, there was a sixfold increase in 16S copy number (P = 0.007) and a 16% rise in numbers of proteobacterial sequences, most notably in potentially pathogenic Haemophilus influenzae (P = 2.7 × 10(-20)), from a preexisting community. These changes occurred only in the sputum microbiome of subjects with COPD and were still evident 42 days after infection. This was in contrast to the temporal stability demonstrated in the microbiome of healthy smokers and nonsmokers.
Conclusions: After rhinovirus infection, there is a rise in bacterial burden and a significant outgrowth of Haemophilus influenzae from the existing microbiota of subjects with COPD. This is not observed in healthy individuals. Our findings suggest that rhinovirus infection in COPD alters the respiratory microbiome and may precipitate secondary bacterial infections.
Figures
Comment in
-
The lung microbiome and viral-induced exacerbations of chronic obstructive pulmonary disease: new observations, novel approaches.Am J Respir Crit Care Med. 2013 Nov 15;188(10):1185-6. doi: 10.1164/rccm.201309-1573ED. Am J Respir Crit Care Med. 2013. PMID: 24236585 No abstract available.
References
-
- Papi A, Bellettato CM, Braccioni F, Romagnoli M, Casolari P, Caramori G, Fabbri LM, Johnston SL. Infections and airway inflammation in chronic obstructive pulmonary disease severe exacerbations. Am J Respir Crit Care Med. 2006;173:1114–1121. - PubMed
-
- Seemungal T, Sykes A ICEAD Contributors. Recent advances in exacerbations of COPD. Thorax. 2008;63:850–852. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
