

ST segment elevations: always a marker of acute myocardial infarction?
- PMID: 23993002
- PMCID: PMC3860734
- DOI: 10.1016/j.ihj.2013.06.013
ST segment elevations: always a marker of acute myocardial infarction?
Abstract
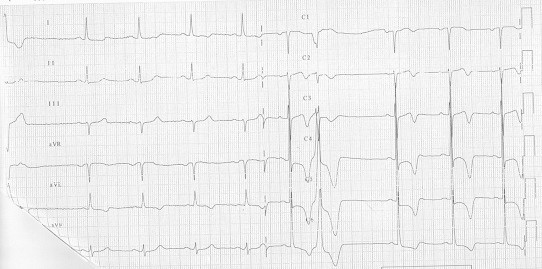
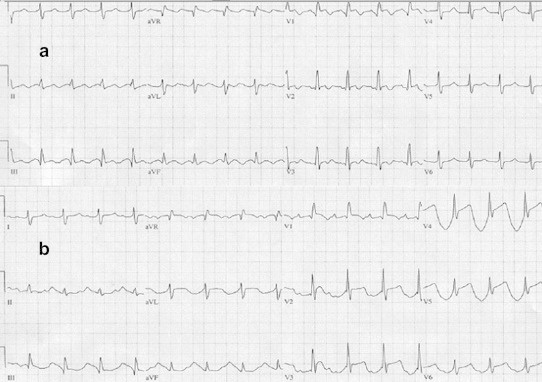
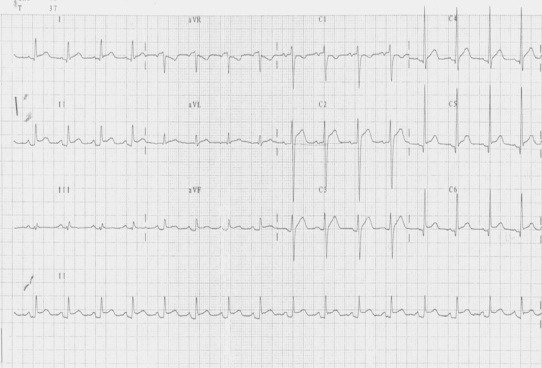
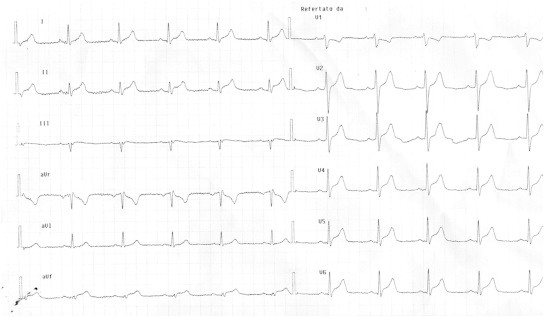
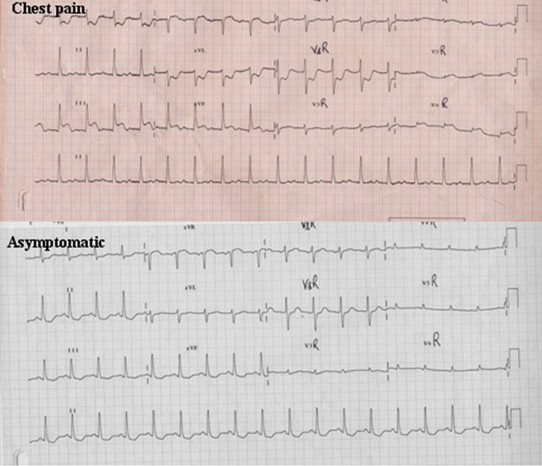
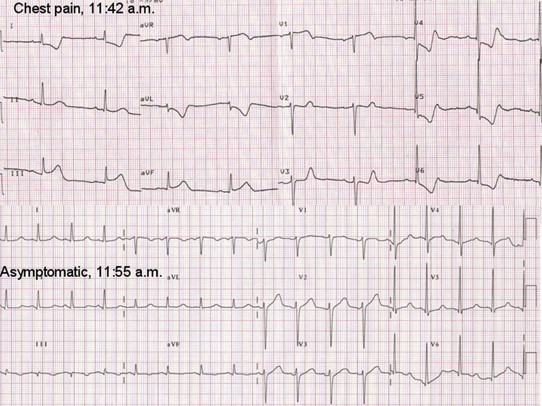
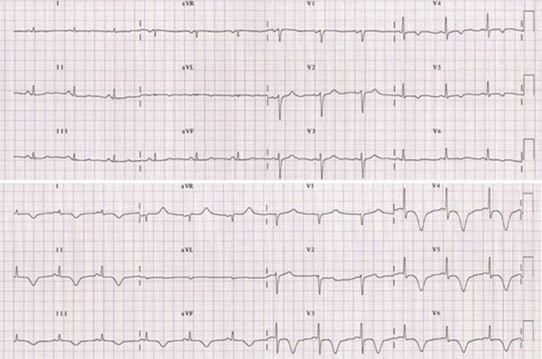
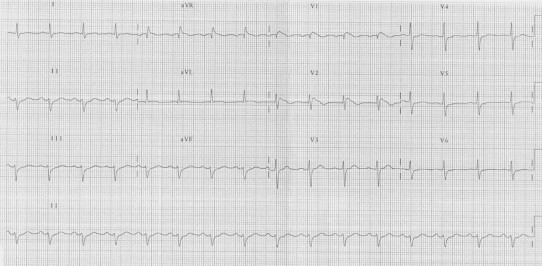
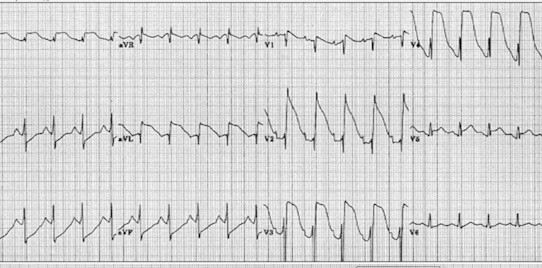
Chest pain is one of the chief presenting complaints among patients attending Emergency department. The diagnosis of acute myocardial infarction may be a challenge. Various tools such as anamnesis, blood sample (with evaluation of markers of myocardial necrosis), ultrasound techniques and coronary computed tomography could be useful. However, the interpretation of electrocardiograms of these patients may be a real concern. The earliest manifestations of myocardial ischemia typically interest T waves and ST segment. Despite the high sensitivity, ST segment deviation has however poor specificity since it may be observed in many other cardiac and non-cardiac conditions. Therefore, when ST-T abnormalities are detected the physicians should take into account many other parameters (such as risk factors, symptoms and anamnesis) and all the other differential diagnoses. The aim of our review is to overview of the main conditions that may mimic a ST segment Elevation Myocardial Infarction (STEMI).
Keywords: Chest pain; Differential diagnosis; ECG; Myocardial infarction; ST segment.
Copyright © 2013 Cardiological Society of India. Published by Elsevier B.V. All rights reserved.
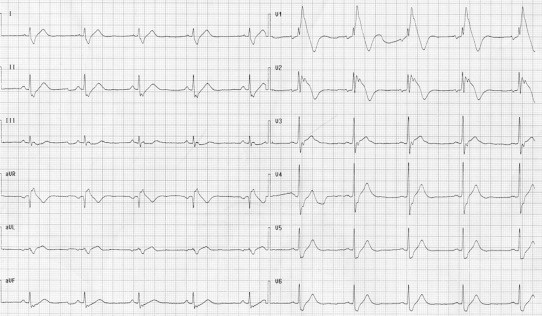
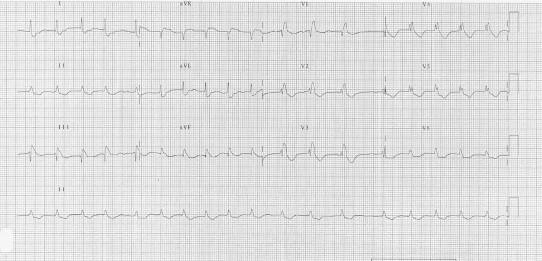
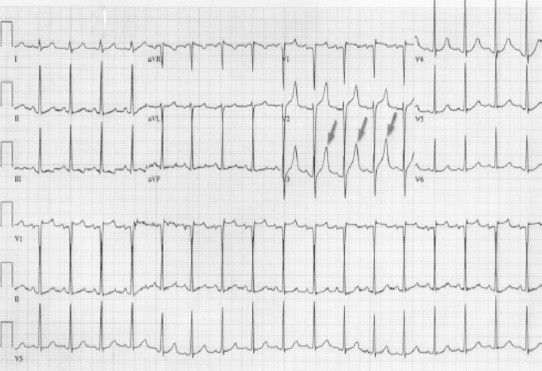
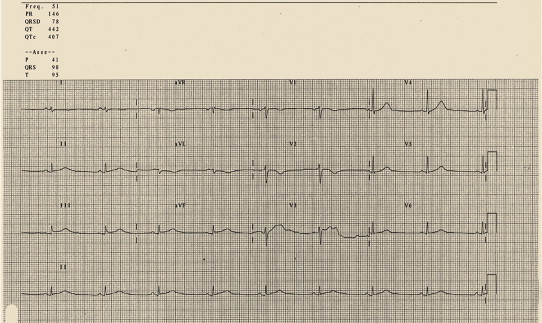
Figures
References
-
- Sharkey S.W., Berger C.R., Brunette D.D., Henry T.D. Impact of the electrocardiogram on the delivery of thrombolytic therapy for acute myocardial infarction. Am J Cardiol. 1994;73:550–553. - PubMed
-
- Green L.S., Lux R.L., Haws C.W., Williams R.R., Hunt S.C., Burgess M.J. Effect of age, sex, and body habitus on QRS and ST-T potential maps of 1100 normal subjects. Circulation. 1985;71:244. - PubMed
-
- Mehta M.C., Jain A.C. Early repolarization on scalar electrocardiogram. Am J Med Sci. 1995;309:305–311. - PubMed
-
- Vacanti L.J. Thoracic pain and early repolarization syndrome at the cardiologic emergency unit. Arq Bras Cardiol. 1996;67:335–338. - PubMed
-
- Fenichell N.N. A long term study of concave RS-T elevation—anormal variant of the electrocardiogram. Angiology. 1962;13:360–366. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
