

Image fusion during vascular and nonvascular image-guided procedures
- PMID: 23993079
- PMCID: PMC3874295
- DOI: 10.1053/j.tvir.2013.02.012
Image fusion during vascular and nonvascular image-guided procedures
Abstract
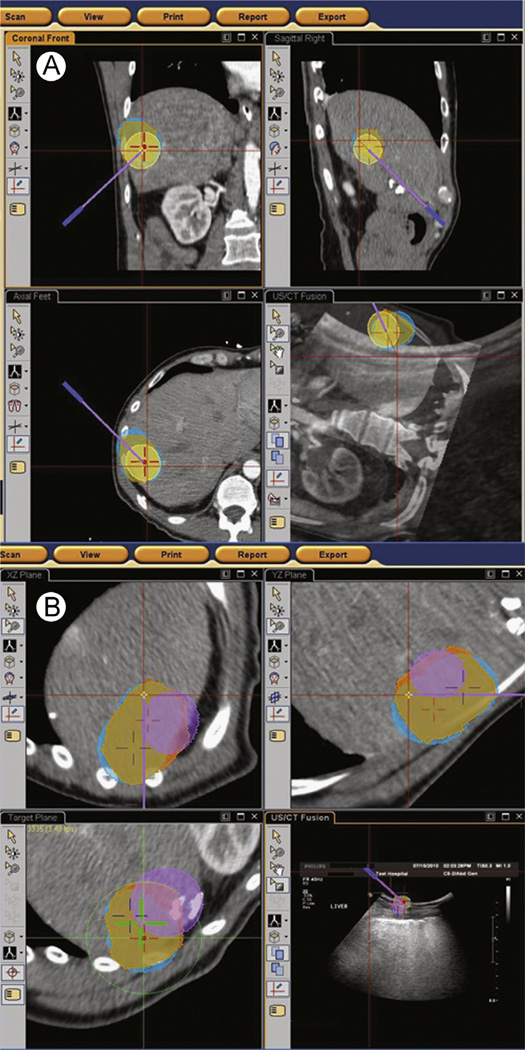
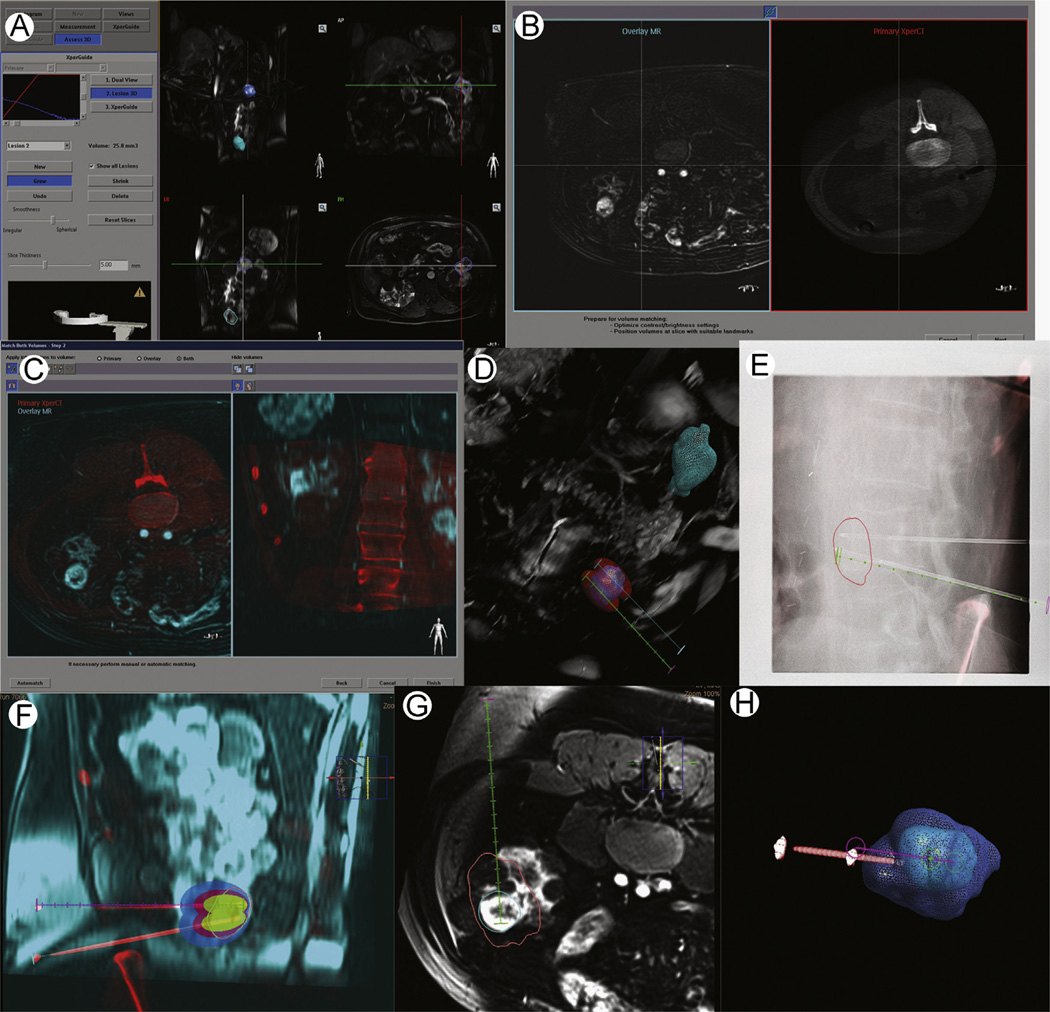
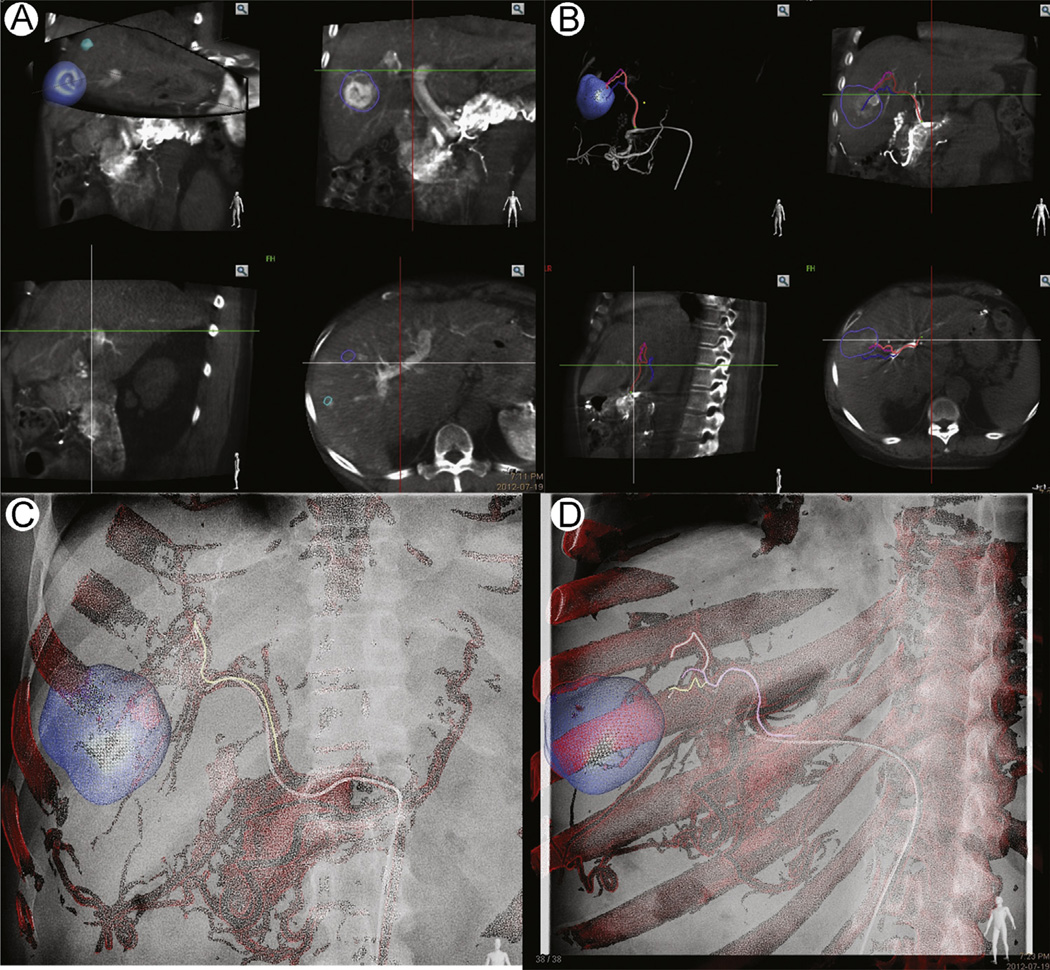
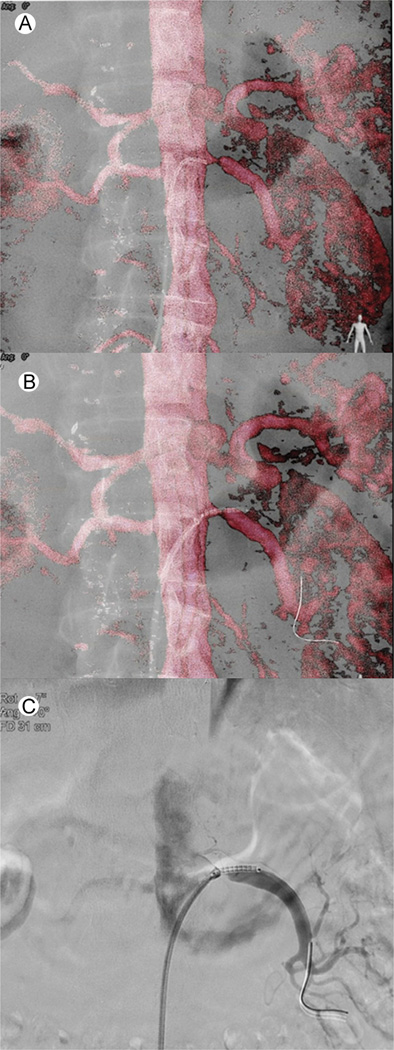
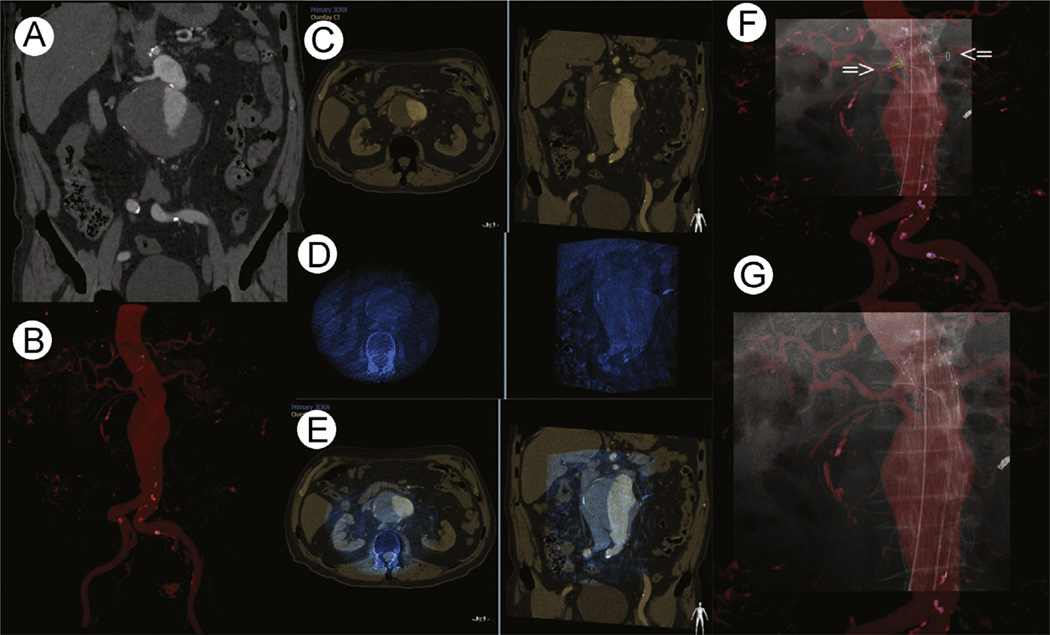
Image fusion may be useful in any procedure where previous imaging such as positron emission tomography, magnetic resonance imaging, or contrast-enhanced computed tomography (CT) defines information that is referenced to the procedural imaging, to the needle or catheter, or to an ultrasound transducer. Fusion of prior and intraoperative imaging provides real-time feedback on tumor location or margin, metabolic activity, device location, or vessel location. Multimodality image fusion in interventional radiology was initially introduced for biopsies and ablations, especially for lesions only seen on arterial phase CT, magnetic resonance imaging, or positron emission tomography/CT but has more recently been applied to other vascular and nonvascular procedures. Two different types of platforms are commonly used for image fusion and navigation: (1) electromagnetic tracking and (2) cone-beam CT. Both technologies would be reviewed as well as their strengths and weaknesses, indications, when to use one vs the other, tips and guidance to streamline use, and early evidence defining clinical benefits of these rapidly evolving, commercially available and emerging techniques.
Keywords: Fusion; cone-beam CT navigation; electromagnetic tracking; navigation.
Published by Elsevier Inc.
Figures
References
-
- Oliveira FP, Tavares JM. Medical image registration: A review. Comput Methods Biomech Biomed Engin. 2012 - PubMed
-
- Zanzonico PB, Nehmeh SA. Introduction to clinical and laboratory (small-animal) image registration and fusion. Conference proceedings : Annual International Conference of the IEEE Engineering in Medicine and Biology Society IEEE Engineering in Medicine and Biology Society Conference. 2006;1:1580–1583. - PubMed
-
- Markelj P, Tomazevic D, Likar B, et al. A review of 3D/2D registration methods for image-guided interventions. Med Image Anal. 2012;16:642–661. - PubMed
-
- Markelj P, Tomazevic D, Likar B, et al. A review of 3D/2D registration methods for image-guided interventions. Med Image Anal. 2012;16:642–661. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
