

Is the lateral transpsoas approach feasible for the treatment of adult degenerative scoliosis?
- PMID: 23996097
- PMCID: PMC4016469
- DOI: 10.1007/s11999-013-3263-5
Is the lateral transpsoas approach feasible for the treatment of adult degenerative scoliosis?
Abstract
Background: Lumbar degenerative scoliosis is a common condition in the elderly. Open traditional surgical approaches are associated with high-morbidity complication rates. Less invasive options may carry fewer risks in this patient population. A minimally disruptive lateral transpsoas retroperitoneal technique to accomplish interbody fusion was developed to avoid the morbidity of traditional open surgery, but this approach as an anterior stand-alone construction has not been reported yet for the treatment of adult degenerative scoliosis.
Questions/purposes: We determined (1) the clinical outcomes (VAS scores for back and leg, Oswestry Disability Index), (2) the radiographic outcomes (Cobb angle, lumbar lordosis, sacral slope, high-grade subsidence, osseous fusion), and (3) the reoperation and complication rates in an older population undergoing this surgical approach.
Methods: Between 2004 and 2008, 62 patients were treated surgically for adult degenerative scoliosis, of whom 46 (74%) were treated with stand-alone lateral lumbar interbody fusion; 11 of these (24%) were lost to followup before 24 months, leaving the records of 35 patients (nine men, 26 women; mean ± SD age, 68 ± 10 years) available for this retrospective review. General indications for this approach included neurogenic claudication and radicular symptoms with history of chronic low-back pain. A total of 107 levels were treated (mean, three; range, one to seven). Clinical and radiographic outcomes were assessed at a followup of 24 months.
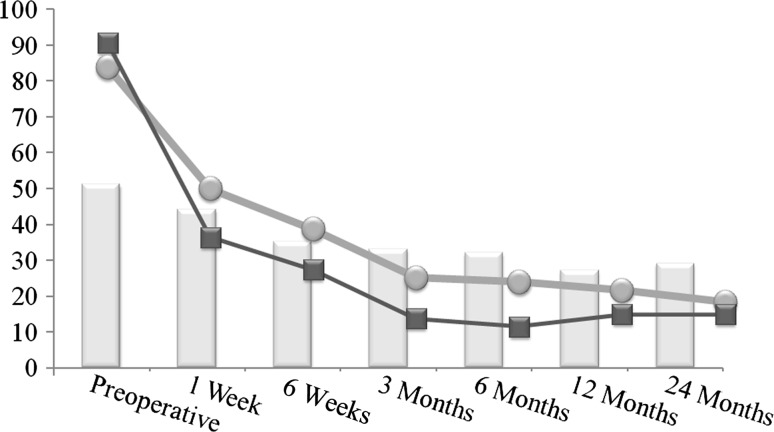
Results: Mean VAS back pain scores improved from 85 mm preoperatively to 27 mm at latest followup (p < 0.001). VAS leg pain scores improved from 91 mm to 24 mm (p < 0.001). Oswestry Disability Index scores improved from 51 to 29 (p < 0.001). Coronal alignment improved from Cobb angles of 21° to 12° (p < 0.001). Lumbar lordosis improved from 33° to 41° (p < 0.001). Sacral slope was enhanced from 28° to 35° (p < 0.001). Fusion rate was 84% at final evaluation. High-grade subsidence was seen in 10 patients (29%). Three patients (9%) needed further surgical intervention.
Conclusions: Use of the lateral approach achieved reasonable coronal and sagittal correction, as well as improvements in pain and function, in mild scoliotic deformities; however, subsidence was a concern, occurring in 29% of patients. Questions still remain regarding the need for additional supplementation or the use of wider cages to prevent subsidence.
Level of evidence: Level IV, therapeutic study. See Instructions for Authors for a complete description of levels of evidence.
Figures

References
-
- Acosta FL, Liu J, Slimack N, Moller D, Fessler R, Koski T. Changes in coronal and sagittal plane alignment following minimally invasive direct lateral interbody fusion for the treatment of degenerative lumbar disease in adults: a radiographic study. J Neurosurg Spine. 2011;15:92–96. doi: 10.3171/2011.3.SPINE10425. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
