

How can socioeconomic inequalities in hospital admissions be explained? A cohort study
- PMID: 23996814
- PMCID: PMC3758975
- DOI: 10.1136/bmjopen-2012-002433
How can socioeconomic inequalities in hospital admissions be explained? A cohort study
Abstract
Objectives: To investigate which antecedent risk factors can explain the social patterning in hospital use.
Design: Prospective cohort study with up to 37 years of follow-up.
Setting: Representative community sample in the West of Scotland.
Participants: 7049 men and 8353 women aged 45-64 years were recruited into the study from the general population between 1972 and 1976 (78% of the eligible population).
Primary and secondary outcome measures: Hospital admissions and bed days by cause and by classification into emergency or non-emergency.
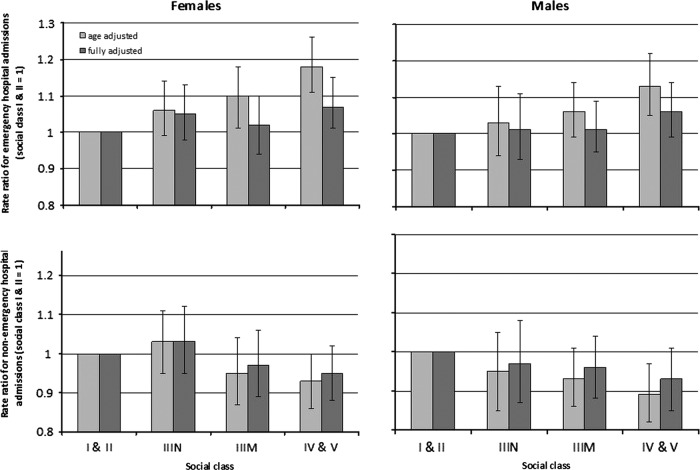
Results: All-cause hospital admission rate ratios (RRs) were not obviously socially patterned for women (RR 1.04, 95% CI 0.98 to 1.10) or men (RR 1.0, 95% CI 0.94 to 1.06) in social classes IV and V compared with social classes I and II. However, cardiovascular disease, coronary heart disease and stroke in women, and respiratory disease for men and women were socially patterned, although this attenuated markedly with the addition of baseline risk factors. Hospital bed days were generally socially patterned and the differences were largely explained by baseline risk factors. The overall RRs of mental health admissions in contrast were socially patterned for women (RR 1.77, 95% CI 1.38 to 2.27) and men (RR 1.51, 95% CI 1.11 to 2.06) in social classes IV and V compared with social classes I and II, but the pattern did not attenuate with the addition of baseline risk factors. Emergency hospital admissions were associated with lower social class, but there was an inverse relationship for non-emergency hospital admissions.
Conclusions: Overall admissions to hospital were only marginally socially patterned, and less than would be expected on the basis of the gradient in baseline risk. However, there was marked social patterning in admissions for mental health problems. Non-emergency hospital admissions were patterned inversely according to risk. Further work is required to explain and address this inequitable gradient in healthcare use.
Keywords: PREVENTIVE MEDICINE; PUBLIC HEALTH.
Figures
Similar articles
-
Socioeconomic status within social class and mortality: a prospective study in middle-aged British men.Int J Epidemiol. 1997 Jun;26(3):532-41. doi: 10.1093/ije/26.3.532. Int J Epidemiol. 1997. PMID: 9222778
-
Occupational class differences in later life hospital use by women who survived to age 80: the Renfrew and Paisley prospective cohort study.Age Ageing. 2015 May;44(3):515-9. doi: 10.1093/ageing/afu184. Epub 2014 Nov 28. Age Ageing. 2015. PMID: 25432982
-
Demographic and socioeconomic inequalities in the risk of emergency hospital admission for violence: cross-sectional analysis of a national database in Wales.BMJ Open. 2016 Aug 24;6(8):e011169. doi: 10.1136/bmjopen-2016-011169. BMJ Open. 2016. PMID: 27558900 Free PMC article.
-
Hospital use by an ageing cohort: an investigation into the association between biological, behavioural and social risk markers and subsequent hospital utilization.J Public Health Med. 1998 Dec;20(4):467-76. doi: 10.1093/oxfordjournals.pubmed.a024804. J Public Health Med. 1998. PMID: 9923956
-
Predicting risk of emergency admission to hospital using primary care data: derivation and validation of QAdmissions score.BMJ Open. 2013 Aug 19;3(8):e003482. doi: 10.1136/bmjopen-2013-003482. BMJ Open. 2013. PMID: 23959760 Free PMC article.
Cited by
-
Patient characteristics associated with risk of first hospital admission and readmission for acute exacerbation of chronic obstructive pulmonary disease (COPD) following primary care COPD diagnosis: a cohort study using linked electronic patient records.BMJ Open. 2016 Jan 22;6(1):e009121. doi: 10.1136/bmjopen-2015-009121. BMJ Open. 2016. PMID: 26801463 Free PMC article.
-
Pushing poverty off limits: quality improvement and the architecture of healthcare values.BMC Med Ethics. 2021 Jul 13;22(1):91. doi: 10.1186/s12910-021-00655-x. BMC Med Ethics. 2021. PMID: 34256744 Free PMC article.
-
Are unmet health related social needs associated with emergency department utilization among Medicare beneficiaries?BMC Health Serv Res. 2025 Mar 31;25(1):477. doi: 10.1186/s12913-025-12554-7. BMC Health Serv Res. 2025. PMID: 40165309 Free PMC article.
-
Socioeconomic and citizenship inequalities in hospitalisation of the adult population in Italy.PLoS One. 2020 Apr 23;15(4):e0231564. doi: 10.1371/journal.pone.0231564. eCollection 2020. PLoS One. 2020. PMID: 32324771 Free PMC article.
-
The influence of socioeconomic deprivation on multimorbidity at different ages: a cross-sectional study.Br J Gen Pract. 2014 Jul;64(624):e440-7. doi: 10.3399/bjgp14X680545. Br J Gen Pract. 2014. PMID: 24982497 Free PMC article.
References
-
- Hart JT. The inverse care law. Lancet 1971;297:405–12 - PubMed
-
- Peen J, Dekker J. Social deprivation and psychiatric service use for different diagnostic groups. Soc Sci Med 2001;53:1–8 - PubMed
-
- Barnett R, Lauer G. Urban deprivation and public hospital admissions in Christchurch, New Zealand, 1990–1997. Health Soc Care Community 2003;11:299–313 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources