

Updated estimate of AQP4-IgG serostatus and disability outcome in neuromyelitis optica
- PMID: 23997151
- PMCID: PMC3795610
- DOI: 10.1212/WNL.0b013e3182a6cb5c
Updated estimate of AQP4-IgG serostatus and disability outcome in neuromyelitis optica
Abstract
Objective: To 1) determine, using contemporary recombinant antigen-based assays, the aquaporin-4 (AQP4)-immunoglobulin G (IgG) detection rate in sequential sera of patients assigned a clinical diagnosis of neuromyelitis optica (NMO) but initially scored negative by tissue-based indirect immunofluorescence (IIF) assay; and 2) evaluate the impact of serostatus on phenotype and outcome.
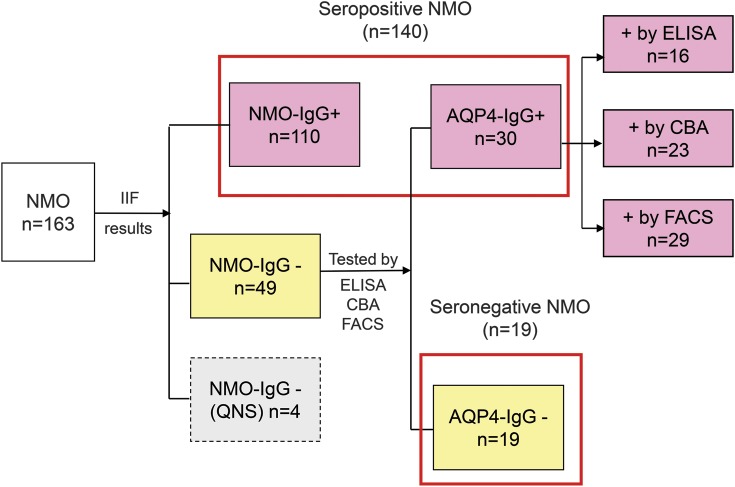
Methods: From Mayo Clinic records (2005-2011), we identified 163 patients with NMO; 110 (67%) were seropositive by IIF and 53 (33%) were scored seronegative. Available stored sera from 49 "seronegative" patients were tested by ELISA, AQP4-transfected cell-based assay, and in-house fluorescence-activated cell sorting assay. Clinical characteristics were compared based on final serostatus.
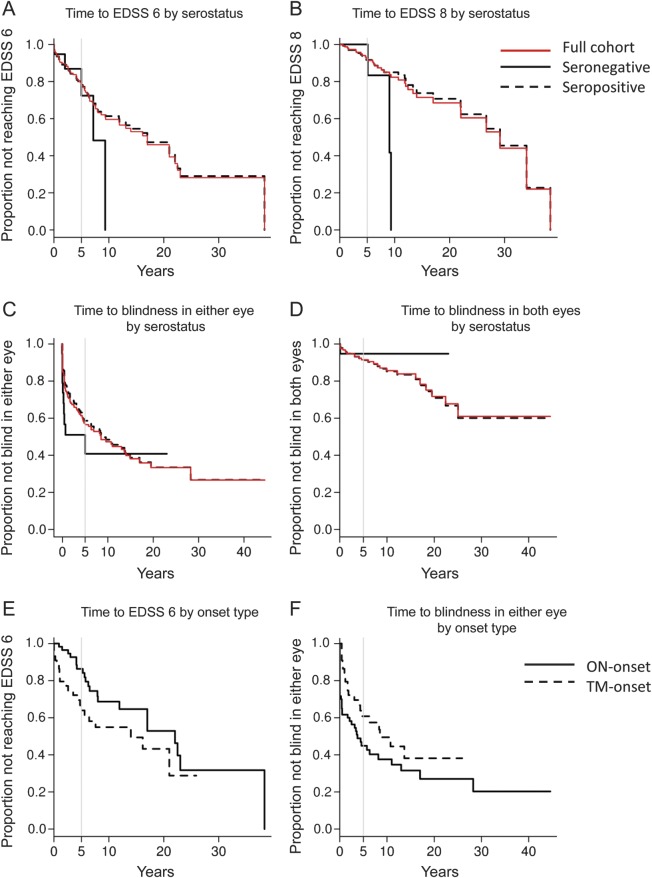
Results: Thirty of the 49 IIF-negative patients (61%) were reclassified as seropositive, yielding an overall AQP4-IgG seropositivity rate of 88% (i.e., 12% seronegative). The fluorescence-activated cell sorting assay improved the detection rate to 87%, cell-based assay to 84%, and ELISA to 79%. The sex ratio (female to male) was 1:1 for seronegatives and 9:1 for seropositives (p < 0.0001). Simultaneous optic neuritis and transverse myelitis as onset attack type (i.e., within 30 days of each other) occurred in 32% of seronegatives and in 3.6% of seropositives (p < 0.0001). Relapse rate, disability outcome, and other clinical characteristics did not differ significantly.
Conclusions: Serological tests using recombinant AQP4 antigen are significantly more sensitive than tissue-based IIF for detecting AQP4-IgG. Testing should precede immunotherapy; if negative, later-drawn specimens should be tested. AQP4-IgG-seronegative NMO is less frequent than previously reported and is clinically similar to AQP4-IgG-seropositive NMO.
Figures
Comment in
-
AQP4 antibody serostatus: Is its luster being lost in the management and pathogenesis of NMO?Neurology. 2013 Oct 1;81(14):1186-8. doi: 10.1212/WNL.0b013e3182a6cc23. Epub 2013 Aug 30. Neurology. 2013. PMID: 23997154 No abstract available.
-
Neuroimmunology: Aquaporin-4-antibody-seronegative neuromyelitis optica is less common than previously thought.Nat Rev Neurol. 2013 Nov;9(11):604. doi: 10.1038/nrneurol.2013.196. Epub 2013 Sep 17. Nat Rev Neurol. 2013. PMID: 24042481 No abstract available.
References
-
- Wingerchuk DM, Hogancamp WF, O'Brien PC, Weinshenker BG. The clinical course of neuromyelitis optica (Devic's syndrome). Neurology 1999;53:1107–1114 - PubMed
-
- Wingerchuk DM, Lennon VA, Lucchinetti CF, Pittock SJ, Weinshenker BG. The spectrum of neuromyelitis optica. Lancet Neurol 2007;6:805–815 - PubMed
-
- Lennon VA, Wingerchuk DM, Kryzer TJ, et al. A serum autoantibody marker of neuromyelitis optica: distinction from multiple sclerosis. Lancet 2004;364:2106–2112 - PubMed
-
- Hayakawa S, Mori M, Okuta A, et al. Neuromyelitis optica and anti-aquaporin-4 antibodies measured by an enzyme-linked immunosorbent assay. J Neuroimmunol 2008;196:181–187 - PubMed
-
- McKeon A, Fryer JP, Apiwattanakul M, et al. Diagnosis of neuromyelitis spectrum disorders: comparative sensitivities and specificities of immunohistochemical and immunoprecipitation assays. Arch Neurol 2009;66:1134–1138 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources