

Initial Antituberculous Regimen with Better Drug Penetration into Cerebrospinal Fluid Reduces Mortality in HIV Infected Patients with Tuberculous Meningitis: Data from an HIV Observational Cohort Study
- PMID: 23997952
- PMCID: PMC3753756
- DOI: 10.1155/2013/242604
Initial Antituberculous Regimen with Better Drug Penetration into Cerebrospinal Fluid Reduces Mortality in HIV Infected Patients with Tuberculous Meningitis: Data from an HIV Observational Cohort Study
Abstract
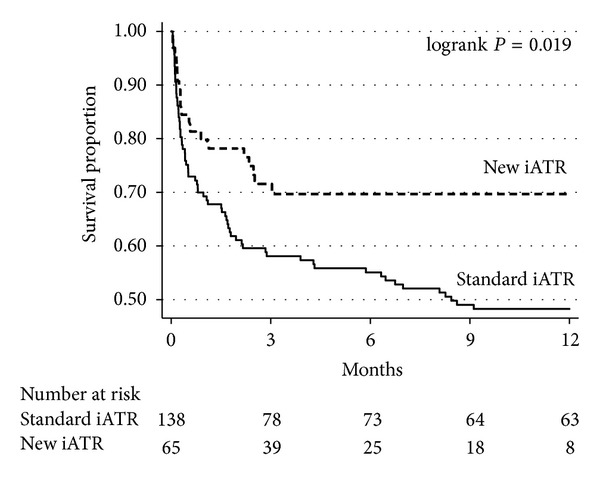
Tuberculous meningitis (TM) is the deadliest form of tuberculosis. Nearly two-thirds of HIV infected patients with TM die, and most deaths occur within one month. Current treatment of TM involves the use of drugs with poor penetration into the cerebro-spinal fluid (CSF). In this study, we present the mortality before and after implementing a new antituberculous regimen (ATR) with a higher drug penetration in CSF than the standard ATR during the initial treatment of TM in an HIV cohort study. The new ATR included levofloxacin, ethionamide, pyrazinamide, and a double dose of rifampicin and isoniazid and was given for a median of 7 days (interquartile range 6-9). The new ATR was associated with an absolute 21.5% (95% confidence interval (CI), 7.3-35.7) reduction in mortality at 12 months. In multivariable analysis, independent factors associated with mortality were the use of the standard ATR versus the new ATR (hazard ratio 2.05; 95% CI, 1.2-3.5), not being on antiretroviral therapy, low CD4 lymphocyte counts, and low serum albumin levels. Our findings suggest that an intensified initial ATR, which likely results in higher concentrations of active drugs in CSF, has a beneficial effect on the survival of HIV-related TM.
Figures

References
-
- World Health Organization. Global tuberculosis control. 2012, http://apps.who.int/iris/bitstream/10665/75938/1/9789241564502_eng.pdf.
-
- Brancusi F, Farrar J, Heemskerk D. Tuberculous meningitis in adults: a review of a decade of developments focusing on prognostic factors for outcome. Future Microbiol. 2012;7:1101–1116. - PubMed
-
- Schutz C, Meintjes G, Almajid F, Wilkinson RJ, Pozniak A. Clinical management of tuberculosis and HIV-1 co-infection. European Respiratory Journal. 2010;36(6):1460–1481. - PubMed
-
- Alvarez-Uria G, Naik PK, Pakam R, Bachu L. Natural history and factors associated with early and delayed mortality in HIV infected patients treated of tuberculosis under directly observed treatment short course (DOTS) strategy: a prospective cohort study in India. Interdisciplinary Perspectives on Infectious Diseases. 2012;2012:9 pages.502012 - PMC - PubMed
-
- Thwaites G, Fisher M, Hemingway C, Scott G, Solomon T, Innes J. British Infection Society guidelines for the diagnosis and treatment of tuberculosis of the central nervous system in adults and children. Journal of Infection. 2009;59(3):167–187. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
