

Management of the patient with incomplete response to PPI therapy
- PMID: 23998978
- PMCID: PMC3761380
- DOI: 10.1016/j.bpg.2013.06.005
Management of the patient with incomplete response to PPI therapy
Abstract
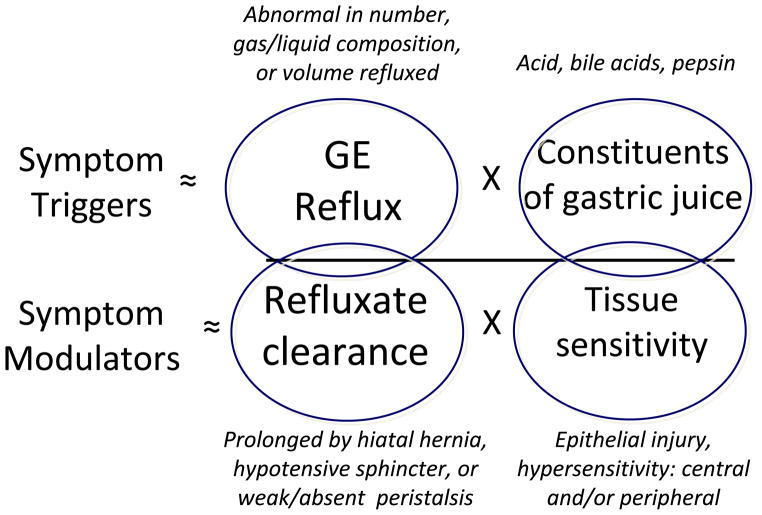
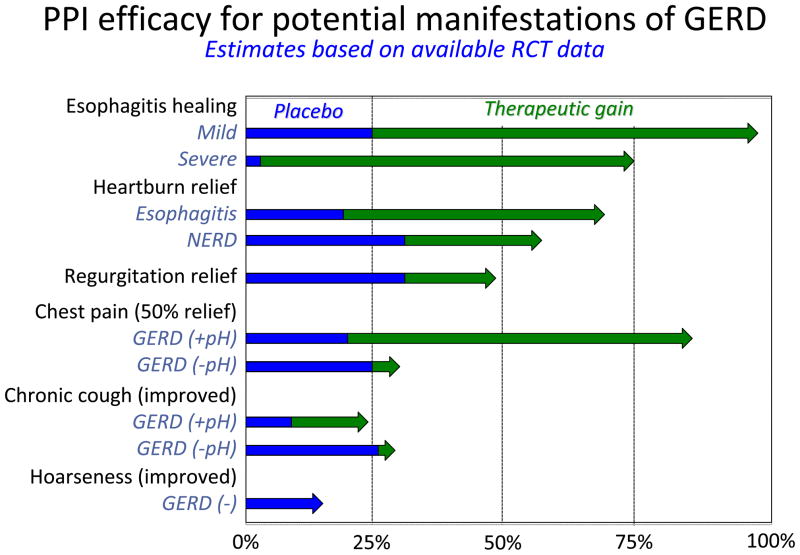
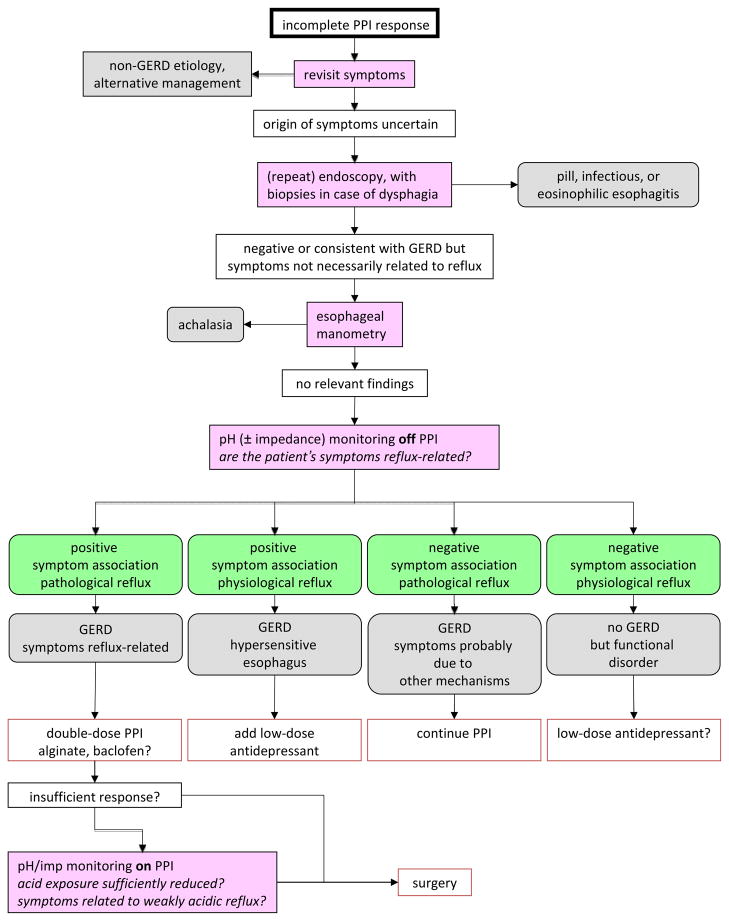
Proton pump inhibitors (PPIs) remove most of the acid from the gastroesophageal refluxate. However, PPIs do not eliminate reflux and the response of specific GERD symptoms to PPI therapy depends on the degree to which acid drives those symptoms. PPIs are progressively less effective for heartburn, regurgitation, chest pain and extra-oesophageal symptoms. Hence, with an incomplete PPI response, obtaining an accurate history, detailing which symptoms are 'refractory' and exactly what evidence exists linking these symptoms to GERD is paramount. Reflux can continue to cause symptoms despite PPI therapy because of persistent acid reflux or weakly acidic reflux. Given these possibilities, diagnostic testing (pH or pH-impedance monitoring) becomes essential. Antireflux surgery is an alternative in patients if a clear relationship is established between persistent symptoms, particularly regurgitation, and reflux. Treating visceral hypersensitivity may also benefit the subset of GERD patients whose symptoms are driven by this mechanism.
Keywords: Ambulatory oesophageal pH monitoring; Ambulatory oesophageal pH-impedance monitoring; Gastroesophageal reflux disease; Oesophagus; Proton pump inhibitors; Visceral hypersensitivity.
Copyright © 2013 Elsevier Ltd. All rights reserved.
Conflict of interest statement
P.J. K serves as a paid consultant for AstraZeneca, Ironwood Pharmaceuticals, Reckitt Benckiser, Glaxo Smith Kline, and Torax. A.J.P.M.S. serves as a paid consultant for Reckitt Benckiser and has received financial support for educational meetings from MMS, Given Imaging and Shire Movetis. G.B. is supported by grants from the Research Foundation - Flanders (FWO) (Odysseus program, G.0905.07) and the agency for Innovation by Science and Technology (IWT), Belgium and has received grant support from Reckitt Benckiser.
Figures
References
-
- Kahrilas PJ, Shaheen NJ, Vaezi M in collaboration with the AGAI Medical Position Panel on GERD management. AGAI medical position statement: management of gastroesophageal reflux disease. Gastroenterology. 2008;135:1383–1391. - PubMed
-
- Numans ME, Lau J, de Wit NJ, Bonis PA. Short-term treatment with proton-pump inhibitors as a test for gastroesophageal reflux disease: a meta-analysis of diagnostic test characteristics. Ann Intern Med. 2004;140:518–27. - PubMed
-
- Kahrilas PJ. Treatment vs management of gastroesophageal reflux disease (editorial) Am J Gastroenterol. 1997;92:1959–1960. - PubMed
-
- Vakil N, Veldhuyzen van Zanten S, Kahrilas P, et al. The Montreal definition and classification of gastro-esophageal reflux disease (GERD) – a global evidence-based consensus. Am J Gastroenterol. 2006;101:1900–20. - PubMed
-
- Sandler RS, Everhart JE, Donowitz M, et al. The burden of selected digestive diseases in the United States. Gastroenterology. 2002;122:1500–11. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
