

A risk prediction score for kidney failure or mortality in rhabdomyolysis
- PMID: 24000014
- PMCID: PMC5152583
- DOI: 10.1001/jamainternmed.2013.9774
A risk prediction score for kidney failure or mortality in rhabdomyolysis
Abstract
Importance: Rhabdomyolysis ranges in severity from asymptomatic elevations in creatine phosphokinase levels to a life-threatening disorder characterized by severe acute kidney injury requiring hemodialysis or continuous renal replacement therapy (RRT).
Objective: To develop a risk prediction tool to identify patients at greatest risk of RRT or in-hospital mortality.
Design, setting, and participants: Retrospective cohort study of 2371 patients admitted between January 1, 2000, and March 31, 2011, to 2 large teaching hospitals in Boston, Massachusetts, with creatine phosphokinase levels in excess of 5000 U/L within 3 days of admission. The derivation cohort consisted of 1397 patients from Massachusetts General Hospital, and the validation cohort comprised 974 patients from Brigham and Women's Hospital.
Main outcomes and measures: The composite of RRT or in-hospital mortality.
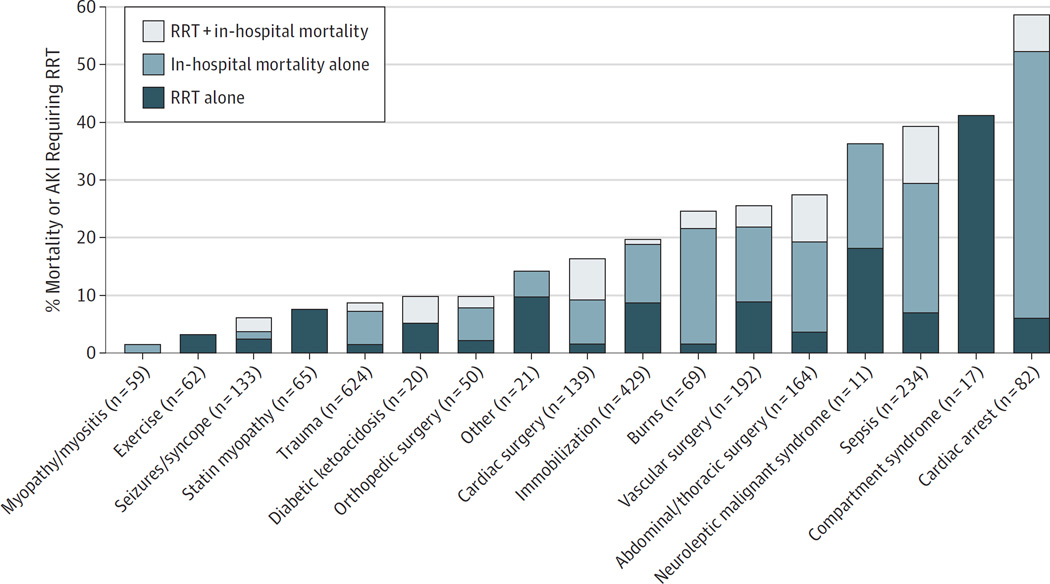
Results: The causes and outcomes of rhabdomyolysis were similar between the derivation and validation cohorts. In total, the composite outcome occurred in 19.0% of patients (8.0% required RRT and 14.1% died during hospitalization). The highest rates of the composite outcome were from compartment syndrome (41.2%), sepsis (39.3%), and following cardiac arrest (58.5%). The lowest rates were from myositis (1.7%), exercise (3.2%), and seizures (6.0%). The independent predictors of the composite outcome were age, female sex, cause of rhabdomyolysis, and values of initial creatinine, creatine phosphokinase, phosphate, calcium, and bicarbonate. We developed a risk-prediction score from these variables in the derivation cohort and subsequently applied it in the validation cohort. The C statistic for the prediction model was 0.82 (95% CI, 0.80-0.85) in the derivation cohort and 0.83 (0.80-0.86) in the validation cohort. The Hosmer-Lemeshow P values were .14 and .28, respectively. In the validation cohort, among the patients with the lowest risk score (<5), 2.3% died or needed RRT. Among the patients with the highest risk score (>10), 61.2% died or needed RRT.
Conclusions and relevance: Outcomes from rhabdomyolysis vary widely depending on the clinical context. The risk of RRT or in-hospital mortality in patients with rhabdomyolysis can be estimated using commonly available demographic, clinical, and laboratory variables on admission.
Figures

Comment in
-
Predicting the outcomes of rhabdomyolysis: a good starting point.JAMA Intern Med. 2013 Oct 28;173(19):1828-9. doi: 10.1001/jamainternmed.2013.9235. JAMA Intern Med. 2013. PMID: 23999843 Free PMC article. No abstract available.
-
Risk factors: predicting prognosis in patients with rhabdomyolysis.Nat Rev Nephrol. 2013 Nov;9(11):637-8. doi: 10.1038/nrneph.2013.207. Epub 2013 Oct 8. Nat Rev Nephrol. 2013. PMID: 24100402
References
-
- Bosch X, Poch E, Grau JM. Rhabdomyolysis and acute kidney injury. N Engl J Med. 2009;361(1):62–72. - PubMed
-
- Melli G, Chaudhry V, Cornblath DR. Rhabdomyolysis: an evaluation of 475 hospitalized patients. Medicine (Baltimore) 2005;84(6):377–385. - PubMed
-
- Delaney KA, Givens ML, Vohra RB. Use of RIFLE criteria to predict the severity and prognosis of acute kidney injury in emergency department patients with rhabdomyolysis. J Emerg Med. 2012;42(5):521–528. - PubMed
-
- de Meijer AR, Fikkers BG, de Keijzer MH, van Engelen BG, Drenth JP. Serum creatine kinase as predictor of clinical course in rhabdomyolysis: a 5-year intensive care survey. Intensive Care Med. 2003;29(7):1121–1125. - PubMed
-
- Waikar SS, Wald R, Chertow GM, et al. Validity of International Classification of Diseases, Ninth Revision, Clinical Modification codes for acute renal failure. J Am Soc Nephrol. 2006;17(6):1688–1694. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
