

Prospective risk factor monitoring reduces intracranial hemorrhage rates in preterm infants
- PMID: 24000297
- PMCID: PMC3752580
- DOI: 10.3238/arztebl.2013.0489
Prospective risk factor monitoring reduces intracranial hemorrhage rates in preterm infants
Abstract
Background: Intracranial hemorrhage occurs in 20% to 25% of neonates born before the 30th week of gestation or weighing less than 1500 grams at birth. These hemorrhages carry a risk of long-term neurocognitive damage. Measures for lowering the incidence of intracranial hemorrhage were evaluated.
Methods: A working group at the University of Ulm, Germany, developed a prospective monitoring program for risk factors and a bundle of measures including altered clinical approaches to delivery, initial care of the neonate in the delivery room immediately after birth, and intensive care in the first few days thereafter. Adherence to these measures was checked once per week. The evaluation was performed prospectively for a period of 23 months (August 2010 to July 2012) with a 31-month period of historical controls (January 2008 to July 2010).
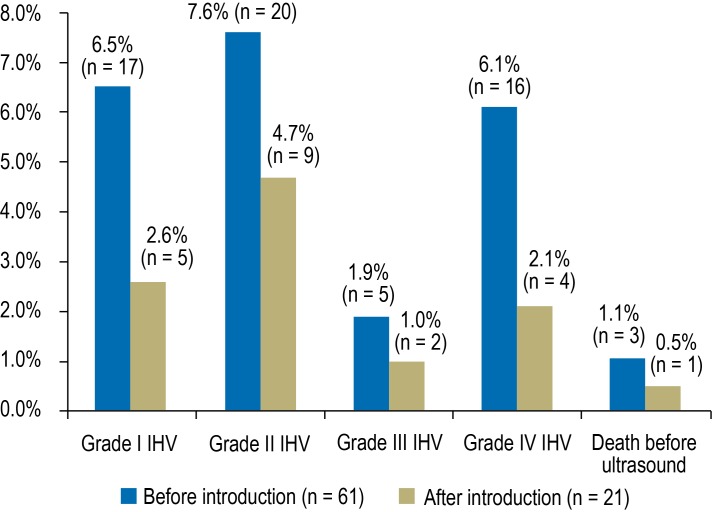
Results: In the reference period before the intervention was introduced, 263 neonates weighing less than 1500 grams and with a median (quartile) gestational age at birth of 27.4 (25.4-29.9) weeks were treated. The incidence of intracranial hemorrhage was 22.1%, and that of high-grade hemorrhage was 9.1%. The mortality was 6.1%, and the rate of survival without brain hemorrhage was 74.5%. After the bundle of preventive measures was introduced, 191 neonates weighing less than 1500 grams and with a median (quartile) gestational age at birth of 28.0 (26.0, 30.3) weeks were treated. The incidence of intracranial hemorrhage dropped to 10.5% (odds ratio [OR] 0.43, 95% confidence interval [CI] 0.25-0.73); the incidence of high-grade hemorrhage dropped to 3.7% (OR 0.36; 95% CI 0.14-0.89). The mortality was no different at 6.3%, and 85.3% of the children survived without a hemorrhage (OR 1.95, 95% CI 1.20-3.15). After statistical adjustment for higher gestational age, the OR for intracranial hemorrhage (IVH) was 0.49 (0.28-0.86) and the probability of survival without IVH improved (OR 1.68, 95% CI 1.01-2.81).
Conclusion: The rate of brain hemorrhage in premature neonates can be considerably lowered by prospective monitoring of risk factors.
Figures
Comment in
-
Prevention at the beginning of life: cerebral hemorrhage in very preterm infants.Dtsch Arztebl Int. 2013 Jul;110(29-30):487-8. doi: 10.3238/arztebl.2013.0487. Dtsch Arztebl Int. 2013. PMID: 24000296 Free PMC article. No abstract available.
-
Consider using heparin.Dtsch Arztebl Int. 2014 Jan 24;111(4):58. doi: 10.3238/arztebl.2014.0058a. Dtsch Arztebl Int. 2014. PMID: 24612498 Free PMC article. No abstract available.
-
In reply.Dtsch Arztebl Int. 2014 Jan 24;111(4):58. doi: 10.3238/arztebl.2014.0058b. Dtsch Arztebl Int. 2014. PMID: 24612499 Free PMC article. No abstract available.
References
-
- Horbar JD, Badger GJ, Carpenter JH, Carpenter F, et al. Trends in mortality and morbidity for very low birth weight infants, 1991-1999. Pediatrics. 2002;110:143–151. - PubMed
-
- Horbar JD, Carpenter JH, Badger GJ, et al. Mortality and neonatal morbidity among infants 501 to 1500 grams from 2000 to 2009. Pediatrics. 2012;129:1019–1026. - PubMed
-
- Allen MC, Cristofalo EA, Kim C. Outcomes of preterm infants: morbidity replaces mortality. Clin Perinatol. 2011;38:441–454. - PubMed
-
- Sherlock RL, Anderson PJ, Doyle LW Victorian Infant Collaborative Study Group. Neurodevelopmental sequelae of intraventricular haemorrhage at 8 years of age in a regional cohort of ELBW/very preterm infants. Early Hum Dev. 2005;81:909–916. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical