

Reversibility of Liver Fibrosis and Inactivation of Fibrogenic Myofibroblasts
- PMID: 24000319
- PMCID: PMC3757252
- DOI: 10.1007/s40139-013-0018-7
Reversibility of Liver Fibrosis and Inactivation of Fibrogenic Myofibroblasts
Abstract
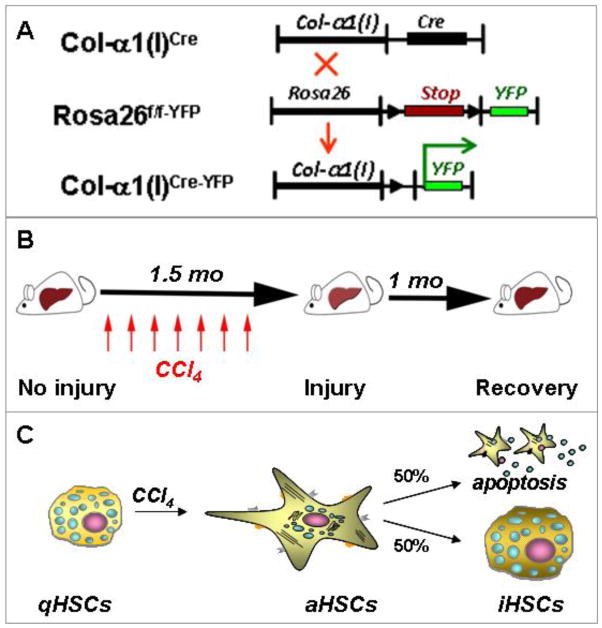
Many studies have demonstrated that hepatic fibrosis is reversible. Regression of liver fibrosis is associated with resorption of fibrous scar and disappearance of collagen producing myofibroblasts. The fate of these myofibroblasts has been recently revealed: Some myofibroblasts undergo senescence and apoptose during reversal of fibrosis, while other myofibroblasts revert to a quiescent-like phenotype. Inactivation of myofibroblasts is a newly described phenomenon1 which now requires mechanistic investigation. Understanding of the mechanism of HSC inactivation upon cessation of fibrogenic stimuli may identify new approaches to revert already existing aHSCs/myofibroblasts into a quiescent-like state. This review summarizes the research on the inactivation of hepatic myofibroblasts.
Keywords: Collagen; HSCs; Hepatic fibrosis; Hepatic stellate cells; Inactivation of myofibroblasts; Pathobiology; Reversibility of liver fibrosis.
Conflict of interest statement
Xiao Liu and Jun Xu declare that they have no conflict of interest.
David A. Brenner holds a patent for inducing inactivation of fibrogenic myofibroblasts. Tatiana Kisseleva holds a patent for inducing inactivation of fibrogenic myofibroblasts, and has received research support from National Institutes of Health/National Institute of Diabetes and Digestive and Kidney Diseases (R56 DK088837-01A10.
Figures
References
-
- Kisseleva T, et al. Myofibroblasts revert to an inactive phenotype during regression of liver fibrosis. Proc Natl Acad Sci U S A. 2012;109:9448–9453. This research article, along with the one by Troeger [30], demonstrated for the first time that aHSCs can inactivate, initiating a new area of research and providing new direction for anti-fibrotic therapy. - PMC - PubMed
-
- Kisseleva T, Brenner DA. Hepatic stellate cells and the reversal of fibrosis. Journal of gastroenterology and hepatology. 2006;21 (Suppl 3):S84–87. - PubMed
-
- Gomperts BN, Strieter RM. Fibrocytes in lung disease. Journal of leukocyte biology. 2007;82:449–456. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources