

Role of Campylobacter jejuni infection in the pathogenesis of Guillain-Barré syndrome: an update
- PMID: 24000328
- PMCID: PMC3755430
- DOI: 10.1155/2013/852195
Role of Campylobacter jejuni infection in the pathogenesis of Guillain-Barré syndrome: an update
Abstract
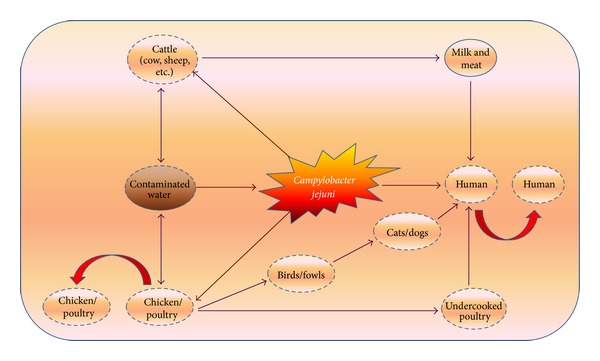
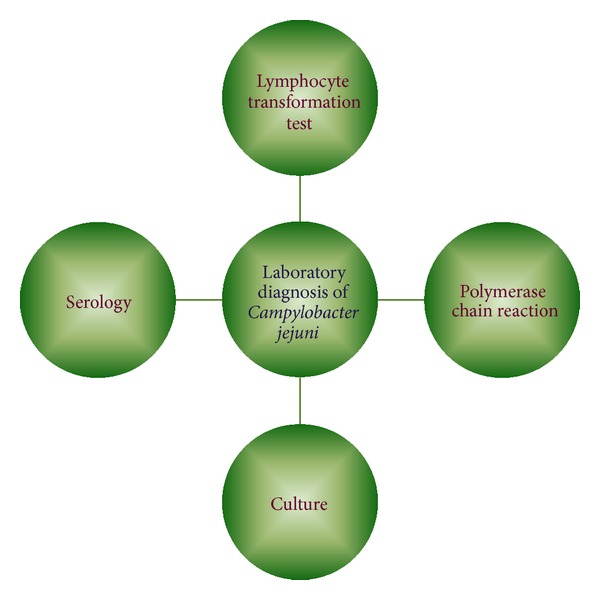
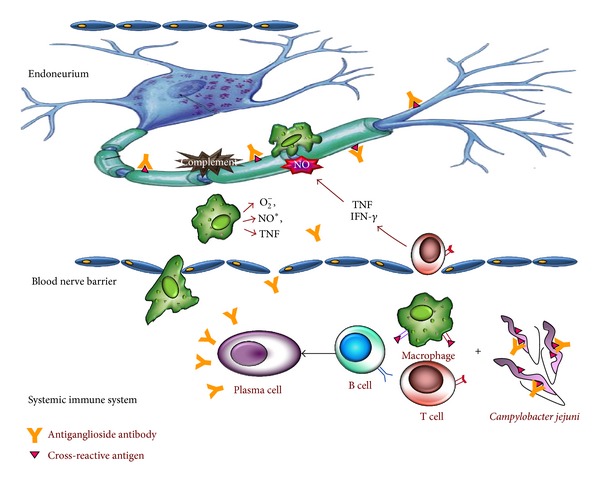
Our current knowledge on Campylobacter jejuni infections in humans has progressively increased over the past few decades. Infection with C. jejuni is the most common cause of bacterial gastroenteritis, sometimes surpassing other infections due to Salmonella, Shigella, and Escherichia coli. Most infections are acquired due to consumption of raw or undercooked poultry, unpasteurized milk, and contaminated water. After developing the diagnostic methods to detect C. jejuni, the possibility to identify the association of its infection with new diseases has been increased. After the successful isolation of C. jejuni, reports have been published citing the occurrence of GBS following C. jejuni infection. Thus, C. jejuni is now considered as a major triggering agent of GBS. Molecular mimicry between sialylated lipooligosaccharide structures on the cell envelope of these bacteria and ganglioside epitopes on the human nerves that generates cross-reactive immune response results in autoimmune-driven nerve damage. Though C. jejuni is associated with several pathologic forms of GBS, axonal subtypes following C. jejuni infection may be more severe. Ample amount of existing data covers a large spectrum of GBS; however, the studies on C. jejuni-associated GBS are still inconclusive. Therefore, this review provides an update on the C. jejuni infections engaged in the pathogenesis of GBS.
Figures
References
-
- Asbury AK, Cornblath DR. Assessment of current diagnostic criteria for Guillain-Barre syndrome. Annals of Neurology. 1990;27:S21–S24. - PubMed
-
- Kuwabara S. Guillain-Barré syndrome: epidemiology, pathophysiology and management. Drugs. 2004;64(6):597–610. - PubMed
-
- Vucic S, Kiernan MC, Cornblath DR. Guillain-Barré syndrome: an update. Journal of Clinical Neuroscience. 2009;16(6):733–741. - PubMed
-
- Sinha S, Prasad KN, Pradhan S, Jain D, Jha S. Detection of preceding Campylobacter jejuni infection by polymerase chain reaction in patients with Guillain-Barré syndrome. Transactions of the Royal Society of Tropical Medicine and Hygiene. 2004;98(6):342–346. - PubMed
-
- Sinha S, Prasad KN, Jain D, Nyati KK, Pradhan S, Agrawal S. Immunoglobulin IgG Fc-receptor polymorphisms and HLA class II molecules in Guillain-Barré syndrome. Acta Neurologica Scandinavica. 2010;122(1):21–26. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
