

Large field, high resolution full-field optical coherence tomography: a pre-clinical study of human breast tissue and cancer assessment
- PMID: 24000981
- PMCID: PMC4527436
- DOI: 10.7785/tcrtexpress.2013.600254
Large field, high resolution full-field optical coherence tomography: a pre-clinical study of human breast tissue and cancer assessment
Abstract
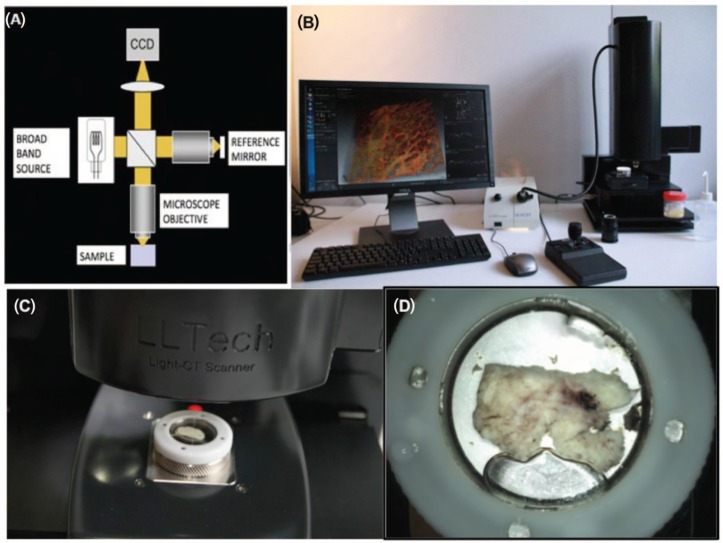
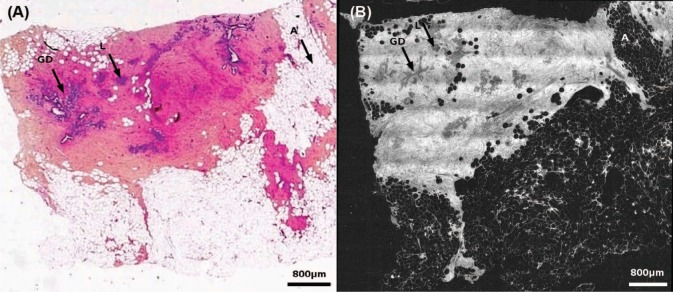
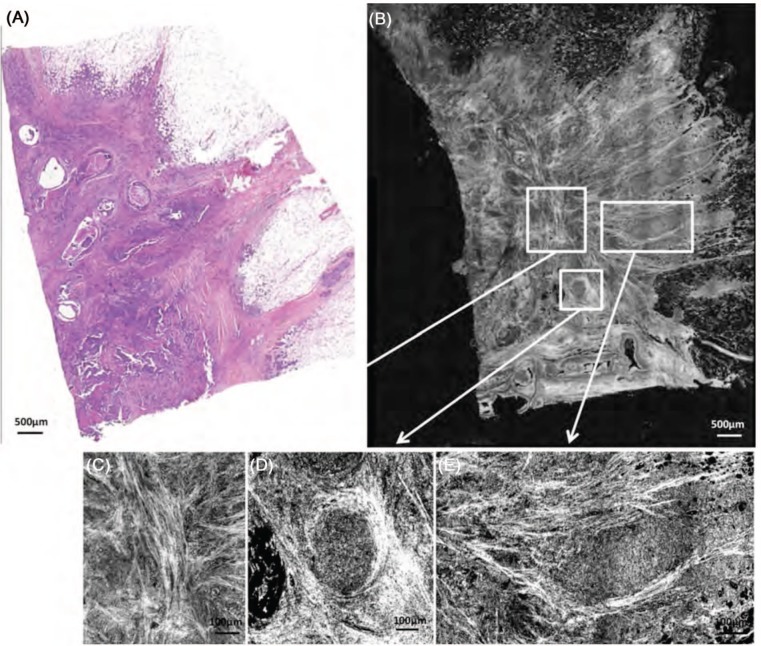
We present a benchmark pilot study in which high-resolution Full-Field Optical Coherence Tomography (FF-OCT) was used to image human breast tissue and is evaluated to assess its ability to aid the pathologist's management of intra-operative diagnoses. FF-OCT imaging safety was investigated and agreement between FF-OCT and routinely prepared histopathological images was evaluated. The compact setup used for this study provides 1 mm3 resolution and 200 mm imaging depth, and a 2.25 cm2 specimen is scanned in about 7 minutes. 75 breast specimens were imaged from 22 patients (21 women, 1 man) with a mean age of 58 (range: 25-83). Pathologists blind diagnosed normal/benign or malignant tissue based on FF-OCT images alone, diagnosis from histopathology followed for comparison. The contrast in the FF-OCT images is generated by intrinsic tissue scattering properties, meaning that no tissue staining or preparation is required. Major architectural features and tissue structures of benign breast tissue, including adipocytes, fibrous stroma, lobules and ducts were characterized. Subsequently, features resulting from pathological modification were characterized and a diagnosis decision tree was developed. Using FF-OCT images, two breast pathologists were able to distinguish normal/benign tissue from lesional with a sensitivity of 94% and 90%, and specificity of 75% and 79% respectively.
Conflict of interest statement
Figures




References
-
- American Cancer Society: Cancer Facts and Figures; 2011.
-
- Silverstein MJ, Recht A, Lagios MD, Bleiweiss IJ, Blumencranz PW, Gizienski T, Harms SE, Harness J, Jackman RJ, Klimberg VS, Kuske R, Levine GM, Linver MN, Rafferty EA, Rugo H, Schilling K, Tripathy D, Whitworth PW, Willey SC. Image-detected breast cancer: state-of-the-art diagnosis and treatment. J Am Coll Surg 209, 504–520 (2009). DOI: 10.1016/j.jamcollsurg.2009.07.006. - PubMed
-
- Cendán JC, Coco D, Copeland EM. Accuracy of intraoperative frozen-section analysis of breast cancer lumpectomy-bed margins. J Am Coll of Surg 201, 194–198 (2005). DOI: 10.1016/j.jamcollsurg.2005.03.014. - PubMed
-
- Nakazawa H, Rosen P, Lane N, Lattes R. Frozen section experience in 3000 cases: accuracy, limitations, and value in residence training. Am J Clin Pathol 49, 41–51 (1968). - PubMed
-
- Olson TP, Harter J, Munoz A, Mahvi DM, Breslin T. Frozen section analysis for intraoperative margin assessment during breast-conserving surgery results in low rates of re-excision and local recurrence. Ann Surg Oncol 14, 2953–2960 (2007). DOI: 10.1245/s10434-007-9437-1. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
