

250 robotic pancreatic resections: safety and feasibility
- PMID: 24002300
- PMCID: PMC4619895
- DOI: 10.1097/SLA.0b013e3182a4e87c
250 robotic pancreatic resections: safety and feasibility
Erratum in
- Ann Surg. 2014 Sep;260(3):566
Abstract
Background and objectives: Computer-assisted robotic surgery allows complex resections and anastomotic reconstructions to be performed with nearly identical standards to open surgery. We applied this technology to a variety of pancreatic resections to assess the safety, feasibility, versatility, and reliability of this technology.
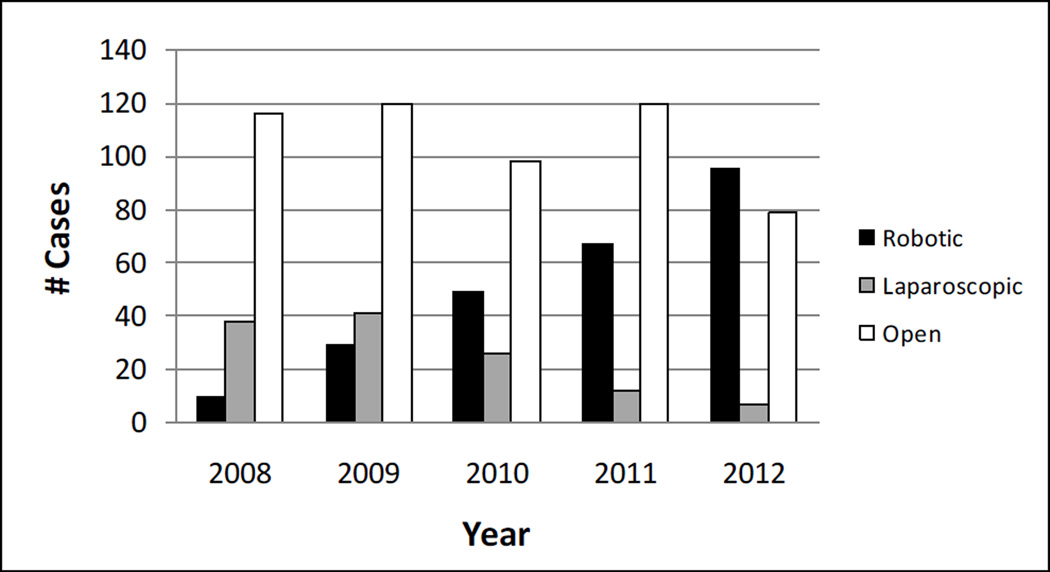
Methods: A retrospective review of a prospective database of robotic pancreatic resections at a single institution between August 2008 and November 2012 was performed. Perioperative outcomes were analyzed.
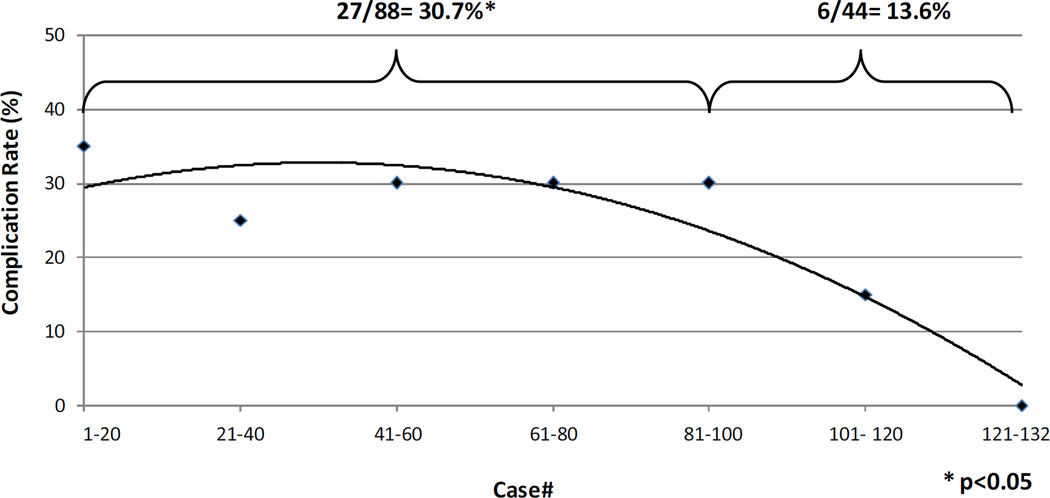
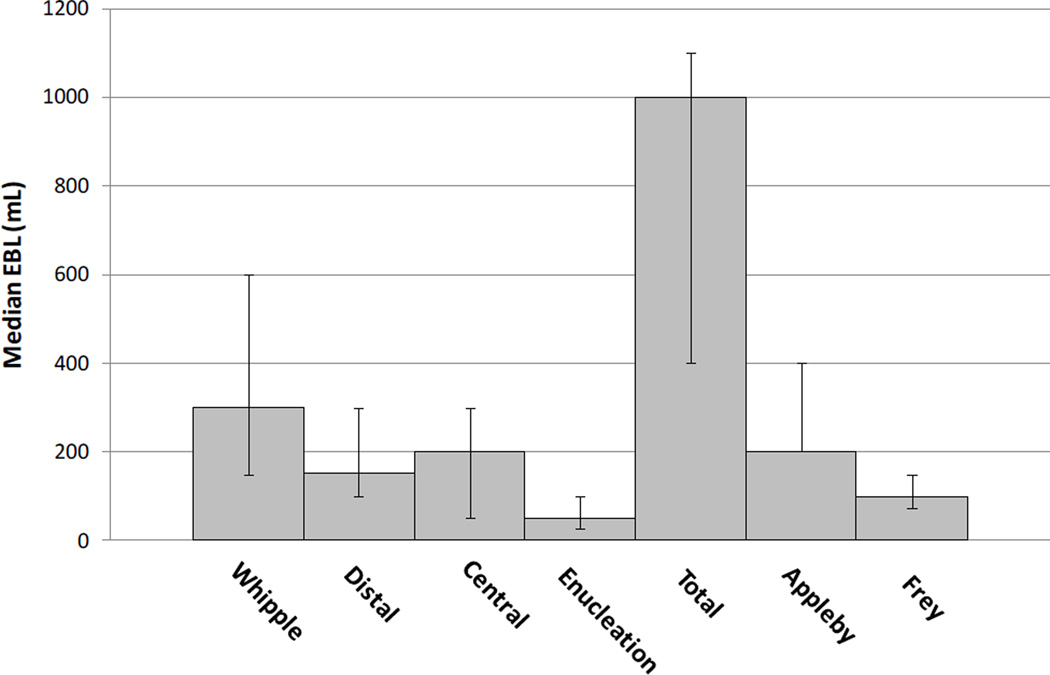
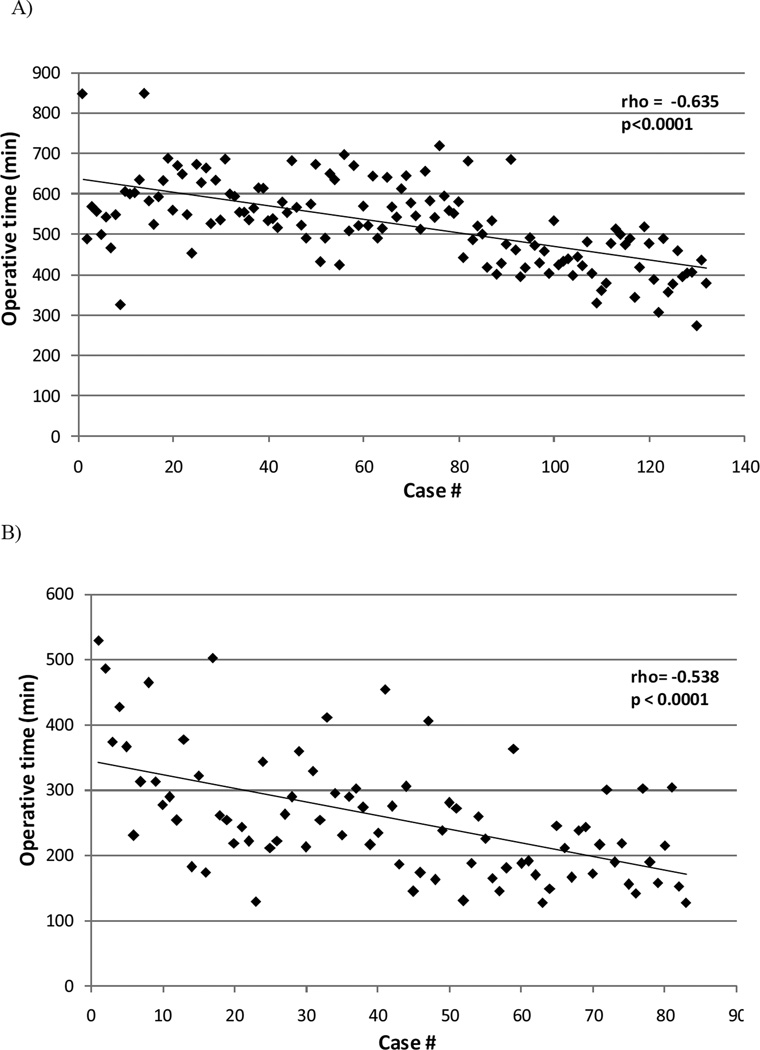
Results: A total of 250 consecutive robotic pancreatic resections were analyzed; pancreaticoduodenectomy (132), distal pancreatectomy (83), central pancreatectomy (13), pancreatic enucleation (10), total pancreatectomy (5), Appleby resection (4), and Frey procedure (3). Thirty-day and 90-day mortality was 0.8% and 2.0%. Rate of Clavien 3 and 4 complications was 14% and 6%. The International Study Group on Pancreatic Fistula grade C fistula rate was 4%. Mean operative time for the 2 most common procedures was 529 ± 103 minutes for pancreaticoduodenectomy and 257 ± 93 minutes for distal pancreatectomy. Continuous improvement in operative times was observed over the course of the experience. Conversion to open procedure was required in 16 patients (6%) (11 with pancreaticoduodenectomy, 2 with distal pancreatectomy, 2 with central pancreatectomy, 1 with total pancreatectomy) for failure to progress (14) and bleeding (2).
Conclusions: This represents to our knowledge the largest series of robotic pancreatic resections. Safety and feasibility metrics including the low incidence of conversion support the robustness of this platform and suggest no unanticipated risks inherent to this new technology. By defining these early outcome metrics, this report begins to establish a framework for comparative effectiveness studies of this platform.
Figures
References
-
- Kendrick ML, Cusati D. Total laparoscopic pancreaticoduodenectomy: feasibility and outcome in an early experience. Arch Surg. 145:19–23. - PubMed
-
- Kendrick ML. Laparoscopic and robotic resection for pancreatic cancer. Cancer J. 18:571–576. - PubMed
-
- Kneuertz PJ, Patel SH, Chu CK, Fisher SB, Maithel SK, Sarmiento JM, Weber SM, Staley CA, Kooby DA. Laparoscopic distal pancreatectomy: trends and lessons learned through an 11-year experience. J Am Coll Surg. 215:167–176. - PubMed
-
- Kooby DA, Gillespie T, Bentrem D, Nakeeb A, Schmidt MC, Merchant NB, Parikh AA, Martin RC, 2nd, Scoggins CR, Ahmad S, Kim HJ, Park J, Johnston F, Strouch MJ, Menze A, Rymer J, McClaine R, Strasberg SM, Talamonti MS, Staley CA, McMasters KM, Lowy AM, Byrd-Sellers J, Wood WC, Hawkins WG. Left-sided pancreatectomy: a multicenter comparison of laparoscopic and open approaches. Ann Surg. 2008;248:438–446. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
