

Indications for anterior lumbar interbody fusion
- PMID: 24002831
- PMCID: PMC6583544
- DOI: 10.1111/os.12048
Indications for anterior lumbar interbody fusion
Abstract
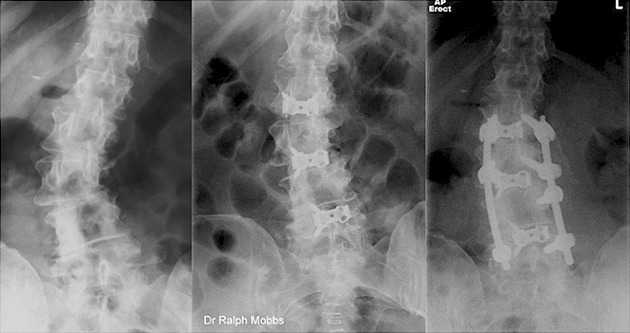
Anterior lumbar interbody fusion (ALIF) has become a widely recognized surgical technique for degenerative pathology of the lumbar spine. Spinal fusion has evolved dramatically ever since the first successful internal fixation by Hadra in 1891 who used a posterior approach to wire adjacent cervical vertebrae in the treatment of fracture-dislocation. Advancements were made to reduce morbidity including bone grafting substitutes, metallic hardware instrumentation and improved surgical technique. The controversy regarding which surgical approach is best for treating various pathologies of the lumbar spine still exists. Despite being an established treatment modality, current indications of ALIF are yet to be clearly defined in the literature. This article discusses the current literature on indications on ALIF surgery.
Keywords: Anterior lumbar interbody fusion; Indications.
© 2013 Chinese Orthopaedic Association and Wiley Publishing Asia Pty Ltd.
Figures

References
-
- Burke PJ. Anterior lumbar interbody fusion. Radiol Technol, 2001, 72: 423–430. - PubMed
-
- Pradhan BB, Nassar JA, Delamarter RB, Wang JC. Single‐level lumbar spine fusion: a comparison of anterior and posterior approaches. J Spinal Disord Tech, 2002, 15: 355–361. - PubMed
-
- van Akkerveeken PF. Anterior lumbar interbody fusion. Acta Orthop Scand Suppl, 1993, 251: 105–107. - PubMed
-
- Shen FH, Samartzis D, Khanna AJ, Anderson DG. Minimally invasive techniques for lumbar interbody fusions. Orthop Clin North Am, 2007, 38: 373–386. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
