

Outcomes of transplantation of livers from donation after circulatory death donors in the UK: a cohort study
- PMID: 24002984
- PMCID: PMC3773642
- DOI: 10.1136/bmjopen-2013-003287
Outcomes of transplantation of livers from donation after circulatory death donors in the UK: a cohort study
Abstract
Objectives: Outcomes of liver transplantations from donation after circulatory death (DCD) donors may be inferior to those achieved with donation after brain death (DBD) donors. The impact of using DCD donors is likely to depend on specific national practices. We compared risk-adjusted graft loss and recipient mortality after transplantation of DCD and DBD livers in the UK.
Design: Prospective cohort study. Multivariable Cox regression and propensity score matching were used to estimate risk-adjusted HR.
Setting: 7 liver transplant centres in the National Health Service (NHS) hospitals in England and Scotland.
Participants: Adults who received a first elective liver transplant between January 2005 and December 2010 who were identified in the UK Liver Transplant Audit.
Interventions: Transplantation of DCD and DBD livers.
Outcomes: Graft loss and recipient mortality.
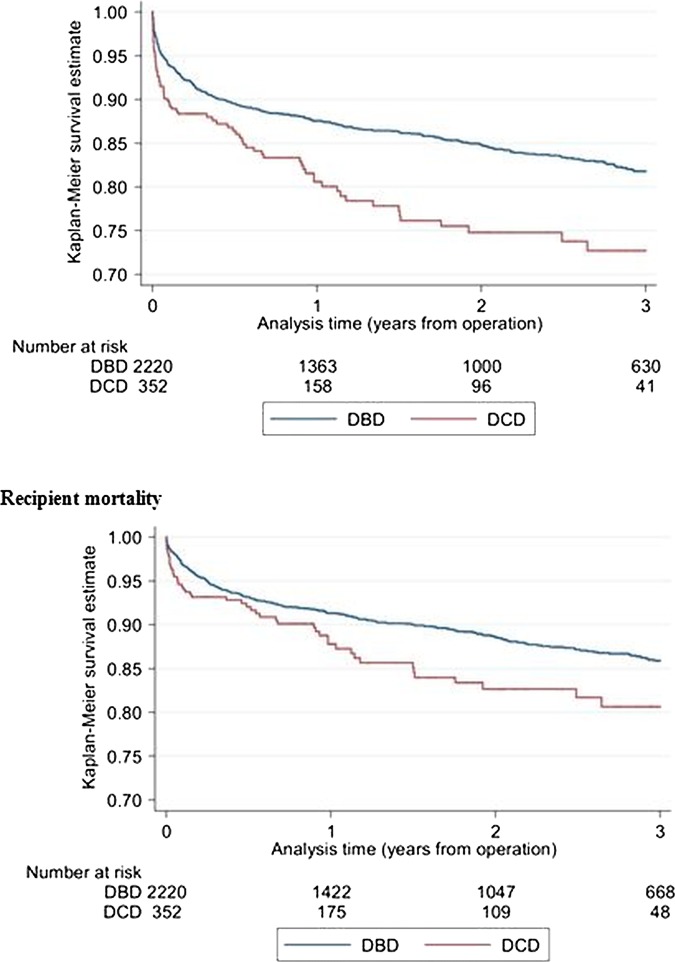
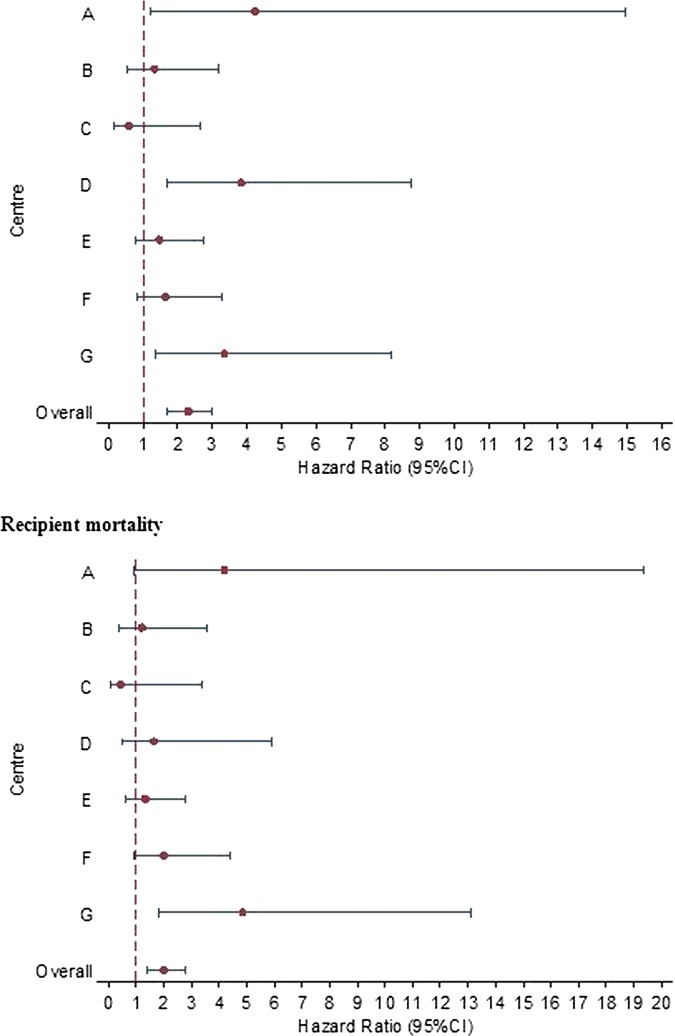
Results: In total, 2572 liver transplants were identified with 352 (14%) from DCD donors. 3-year graft loss (95% CI) was higher with DCD livers (27.3%, 21.8% to 33.9%) than with DBD livers (18.2%, 16.4% to 20.2%). After adjustment with regression, HR for graft loss was 2.3 (1.7 to 3.0). Similarly, 3-year mortality was higher with DCD livers (19.4%, 14.5% to 25.6%) than with DBD livers (14.1%, 12.5% to 16.0%) with an adjusted HR of 2.0 (1.4 to 2.8). Propensity score matching gave similar results. Centre-specific adjusted HRs for graft loss and recipient mortality seemed to differ among transplant centres, although statistical evidence is weak (p value for interaction 0.08 and 0.24, respectively).
Conclusions: Graft loss and recipient mortality were about twice as high with DCD livers as with DBD livers in the UK. Outcomes after DCD liver transplantation may vary between centres. These results should inform policies for the use of DCD livers.
Keywords: EPIDEMIOLOGY; STATISTICS & RESEARCH METHODS; Transplantation.
Figures
References
-
- Kootstra G, Daemen JH, Oomen AP. Categories of non-heart-beating donors. Transplant Proc 1995;27:2893–4 - PubMed
-
- Jimenez-Galanes S, Meneu-Diaz MJ, Elola-Olaso AM, et al. Liver transplantation using uncontrolled non-heart-beating donors under normothermic extracorporeal membrane oxygenation. Liver Transpl 2009;15:1110–18 - PubMed
-
- Thuluvath PJ, Guidinger MK, Fung JJ, et al. Liver transplantation in the United States, 1999–2008. Am J Transplant 2010;10(4 Pt 2):1003–19 - PubMed
-
- Dominguez-Gil B, Haase-Kromwijk B, Van Leiden H, et al. Current situation of donation after circulatory death in European countries. Transpl Int 2011;24:676–86 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources